Horeczko Timothy, Green Jeffrey P, Panacek Edward A
University of California Los Angeles, Department of Emergency Medicine, Torrance, California.
University of California Davis, Department of Emergency Medicine, Sacramento, California.
West J Emerg Med. 2014 May;15(3):329-36. doi: 10.5811/westjem.2013.9.18064. Epub 2014 Feb 19.
Consensus guidelines recommend sepsis screening for adults with systemic inflammatory response syndrome (SIRS), but the epidemiology of SIRS among adult emergency department (ED) patients is poorly understood. Recent emphasis on cost-effective, outcomes-based healthcare prompts the evaluation of the performance of large-scale efforts such as sepsis screening. We studied a nationally representative sample to clarify the epidemiology of SIRS in the ED and subsequent category of illness.
This was a retrospective analysis of ED visits by adults from 2007 to 2010 in the National Hospital Ambulatory Medical Care Survey (NHAMCS). We estimated the incidence of SIRS using initial ED vital signs and a Bayesian construct to estimate white blood cell count based on test ordering. We report estimates with Bayesian modified credible intervals (mCIs).
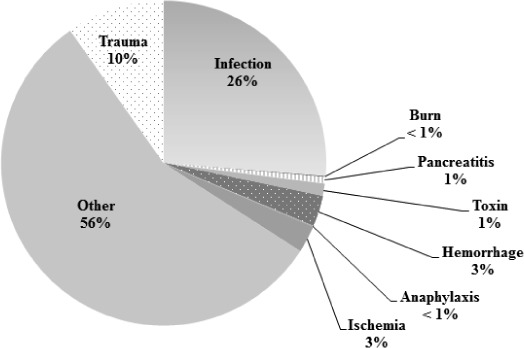
We used 103,701 raw patient encounters in NHAMCS to estimate 372,844,465 ED visits over the 4-year period. The moderate estimate of SIRS in the ED was 17.8% (95% mCI: 9.7 to 26%). This yields a national moderate estimate of approximately 16.6 million adult ED visits with SIRS per year. Adults with and without SIRS had similar demographic characteristics, but those with SIRS were more likely to be categorized as emergent in triage (17.7% versus 9.9%, p<0.001), stay longer in the ED (210 minutes versus 153 minutes, p<0.0001), and were more likely to be admitted (31.5% versus 12.5%, p<0.0001). Infection accounted for only 26% of SIRS patients. Traumatic causes of SIRS comprised 10% of presentations; other traditional categories of SIRS were rare.
SIRS is very common in the ED. Infectious etiologies make up only a quarter of adult SIRS cases. SIRS may be more useful if modified by clinician judgment when used as a screening test in the rapid identification and assessment of patients with the potential for sepsis. [West J Emerg Med. 2014;15(3):329-336.].
共识指南建议对患有全身炎症反应综合征(SIRS)的成年人进行脓毒症筛查,但对于急诊科(ED)成年患者中SIRS的流行病学情况了解甚少。近期对具有成本效益的、基于结果的医疗保健的重视促使人们对脓毒症筛查等大规模举措的效果进行评估。我们研究了一个具有全国代表性的样本,以阐明急诊科中SIRS的流行病学情况及后续疾病类别。
这是一项对2007年至2010年全国医院门诊医疗护理调查(NHAMCS)中成年患者急诊就诊情况的回顾性分析。我们利用急诊科初始生命体征以及一种基于检验医嘱来估计白细胞计数的贝叶斯模型来估计SIRS的发病率。我们报告带有贝叶斯修正可信区间(mCIs)的估计值。
我们利用NHAMCS中的103,701份原始患者就诊记录来估计这4年期间的372,844,465次急诊就诊情况。急诊科中SIRS的中度估计值为17.8%(95% mCI:9.7%至26%)。由此得出全国范围内每年约有1660万成年急诊患者患有SIRS的中度估计值。患有和未患有SIRS的成年人在人口统计学特征上相似,但患有SIRS的患者在分诊时更有可能被归类为紧急情况(17.7%对9.9%,p<0.001),在急诊科停留时间更长(210分钟对153分钟,p<0.0001),并且更有可能被收治(31.5%对12.5%,p<0.0001)。感染仅占SIRS患者的26%。SIRS的创伤性病因占就诊病例的10%;其他传统类型的SIRS很少见。
SIRS在急诊科非常常见。感染性病因仅占成年SIRS病例的四分之一。在快速识别和评估有脓毒症可能的患者时,若将SIRS作为筛查试验并结合临床医生的判断,可能会更有用。[《西方急诊医学杂志》。2014年;15(3):329 - 336。]