Askim Åsa, Moser Florentin, Gustad Lise T, Stene Helga, Gundersen Maren, Åsvold Bjørn Olav, Dale Jostein, Bjørnsen Lars Petter, Damås Jan Kristian, Solligård Erik
Clinic of Anesthesia and Intensive Care, St Olav University Hospital, Trondheim, Norway.
Department of Circulation and Medical Imaging, NTNU, Norwegian University of Science and Technology, Po box 8905, N-7491, Trondheim, Norway.
Scand J Trauma Resusc Emerg Med. 2017 Jun 9;25(1):56. doi: 10.1186/s13049-017-0399-4.
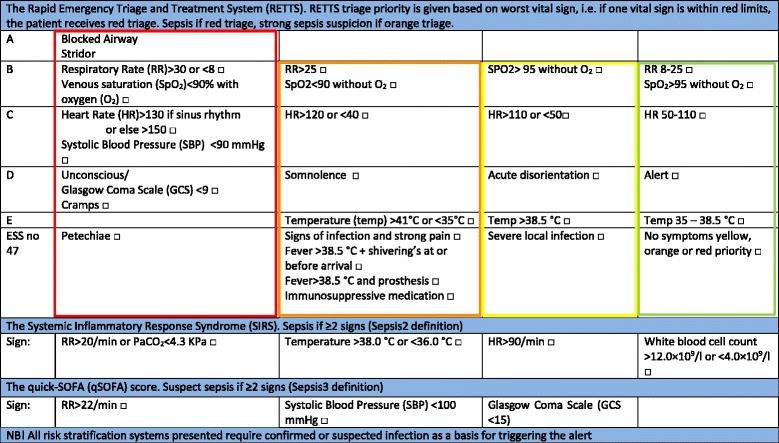
We aimed to evaluate the clinical usefulness of qSOFA as a risk stratification tool for patients admitted with infection compared to traditional SIRS criteria or our triage system; the Rapid Emergency Triage and Treatment System (RETTS).
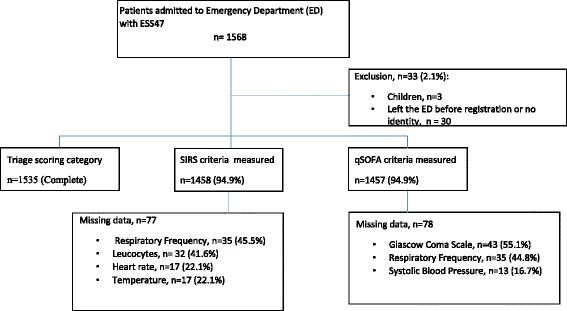
The study was an observational cohort study performed at one Emergency Department (ED) in an urban university teaching hospital in Norway, with approximately 20,000 visits per year. All patients >16 years presenting with symptoms or clinical signs suggesting an infection (n = 1535) were prospectively included in the study from January 1 to December 31, 2012. At arrival in the ED, vital signs were recorded and all patients were triaged according to RETTS vital signs, presenting infection, and sepsis symptoms. These admission data were also used to calculate qSOFA and SIRS. Treatment outcome was later retrieved from the patients' electronic records (EPR) and mortality data from the Norwegian population registry.
Of the 1535 admitted patients, 108 (7.0%) fulfilled the Sepsis2 criteria for severe sepsis. The qSOFA score ≥2 identified only 33 (sensitivity 0.32, specificity 0.98) of the patients with severe sepsis, whilst the RETTS-alert ≥ orange identified 92 patients (sensitivity 0.85, specificity 0.55). Twenty-six patients died within 7 days of admission; four (15.4%) of them had a qSOFA ≥2, and 16 (61.5%) had RETTS ≥ orange alert. Of the 68 patients that died within 30 days, only eight (11.9%) scored ≥2 on the qSOFA, and 45 (66.1%) had a RETTS ≥ orange alert.
In order to achieve timely treatment for sepsis, a sensitive screening tool is more important than a specific one. Our study is the fourth study were qSOFA finds few of the sepsis cases in prehospital or at arrival to the ED. We add information on the RETTS triage system, the two highest acuity levels together had a high sensitivity (85%) for identifying sepsis at arrival to the ED - and thus, RETTS should not be replaced by qSOFA as a screening and trigger tool for sepsis at arrival.
In this observational cohort study, qSOFA failed to identify two thirds of the patients admitted to an ED with severe sepsis. Further, qSOFA failed to be a risk stratification tool as the sensitivity to predict 7-day and 30-day mortality was low. The sensitivity was poorer than the other warning scores already in use at the study site, RETTS-triage and the SIRS criteria.
我们旨在评估与传统全身炎症反应综合征(SIRS)标准或我们的分诊系统——快速急诊分诊与治疗系统(RETTS)相比,qSOFA作为感染入院患者风险分层工具的临床实用性。
本研究是一项观察性队列研究,在挪威一所城市大学教学医院的一个急诊科进行,每年约有20000人次就诊。2012年1月1日至12月31日,前瞻性纳入所有年龄>16岁、出现提示感染症状或体征的患者(n = 1535)。到达急诊科时,记录生命体征,并根据RETTS生命体征、出现的感染及脓毒症症状对所有患者进行分诊。这些入院数据也用于计算qSOFA和SIRS。随后从患者电子病历(EPR)中获取治疗结果,并从挪威人口登记处获取死亡率数据。
1535例入院患者中,108例(7.0%)符合脓毒症2标准的严重脓毒症。qSOFA评分≥2仅识别出33例(敏感性0.32,特异性0.98)严重脓毒症患者,而RETTS警报≥橙色识别出92例患者(敏感性0.85,特异性0.55)。26例患者在入院7天内死亡;其中4例(15.4%)qSOFA≥2,16例(61.5%)RETTS≥橙色警报。在30天内死亡的68例患者中,只有8例(11.9%)qSOFA评分≥2,45例(66.1%)RETTS≥橙色警报。
为了实现脓毒症的及时治疗,一个敏感的筛查工具比一个特异的工具更重要。我们的研究是第四项发现qSOFA在院前或到达急诊科时发现的脓毒症病例很少的研究。我们补充了关于RETTS分诊系统的信息,两个最高 acuity 级别一起对到达急诊科时识别脓毒症具有较高的敏感性(85%)——因此,RETTS不应被qSOFA取代作为到达时脓毒症的筛查和触发工具。
在这项观察性队列研究中,qSOFA未能识别三分之二入住急诊科的严重脓毒症患者。此外,qSOFA未能成为一种风险分层工具,因为其预测7天和30天死亡率的敏感性较低。其敏感性比研究地点已在使用的其他预警评分——RETTS分诊和SIRS标准更差。