Collins George Benjamin, Tan Tien Jin, Gifford John, Tan Andrew
Addenbrooke's Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge Biomedical Campus, Hills Road, Cambridge, CB2 0QQ, UK,
Emerg Radiol. 2014 Dec;21(6):589-95. doi: 10.1007/s10140-014-1243-z. Epub 2014 May 31.
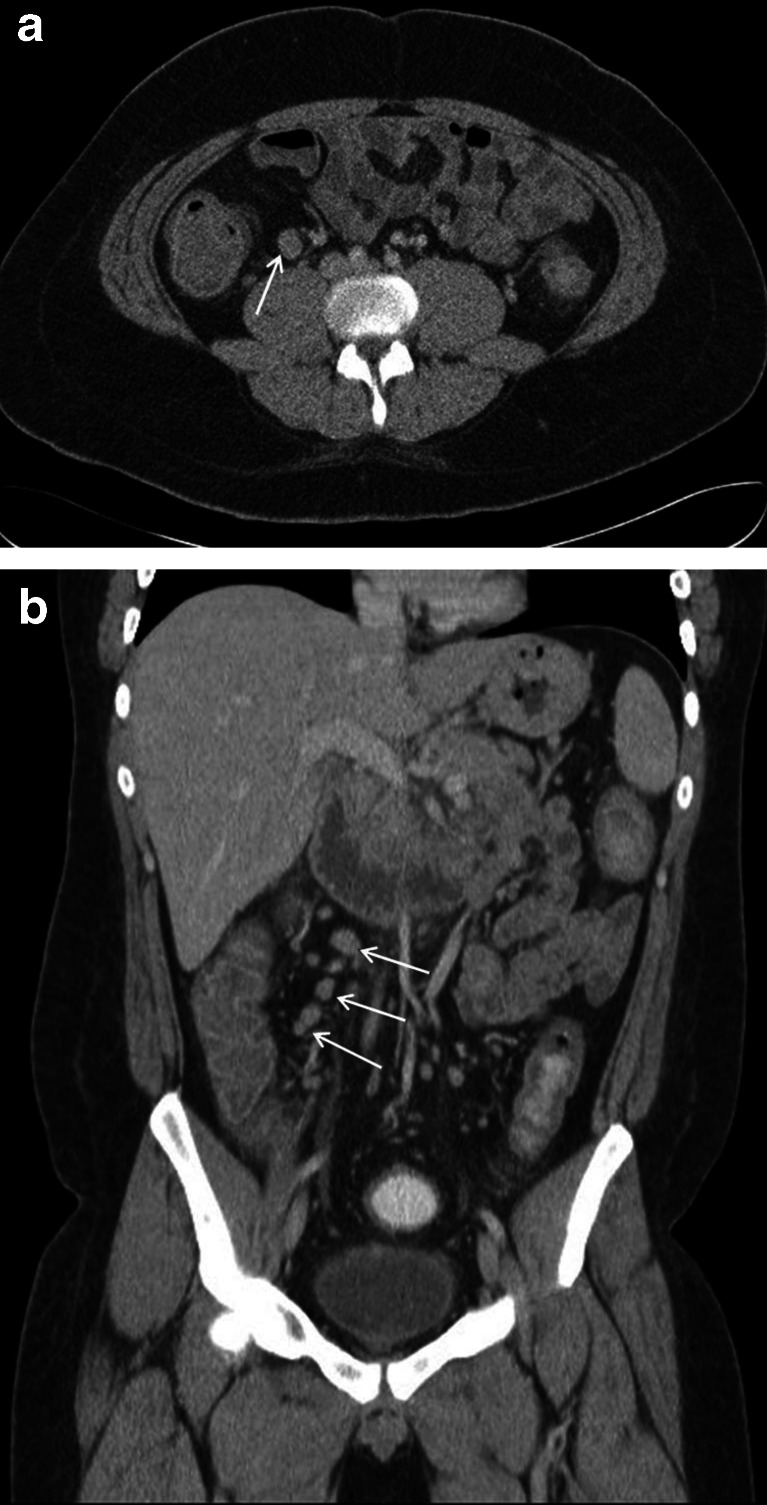
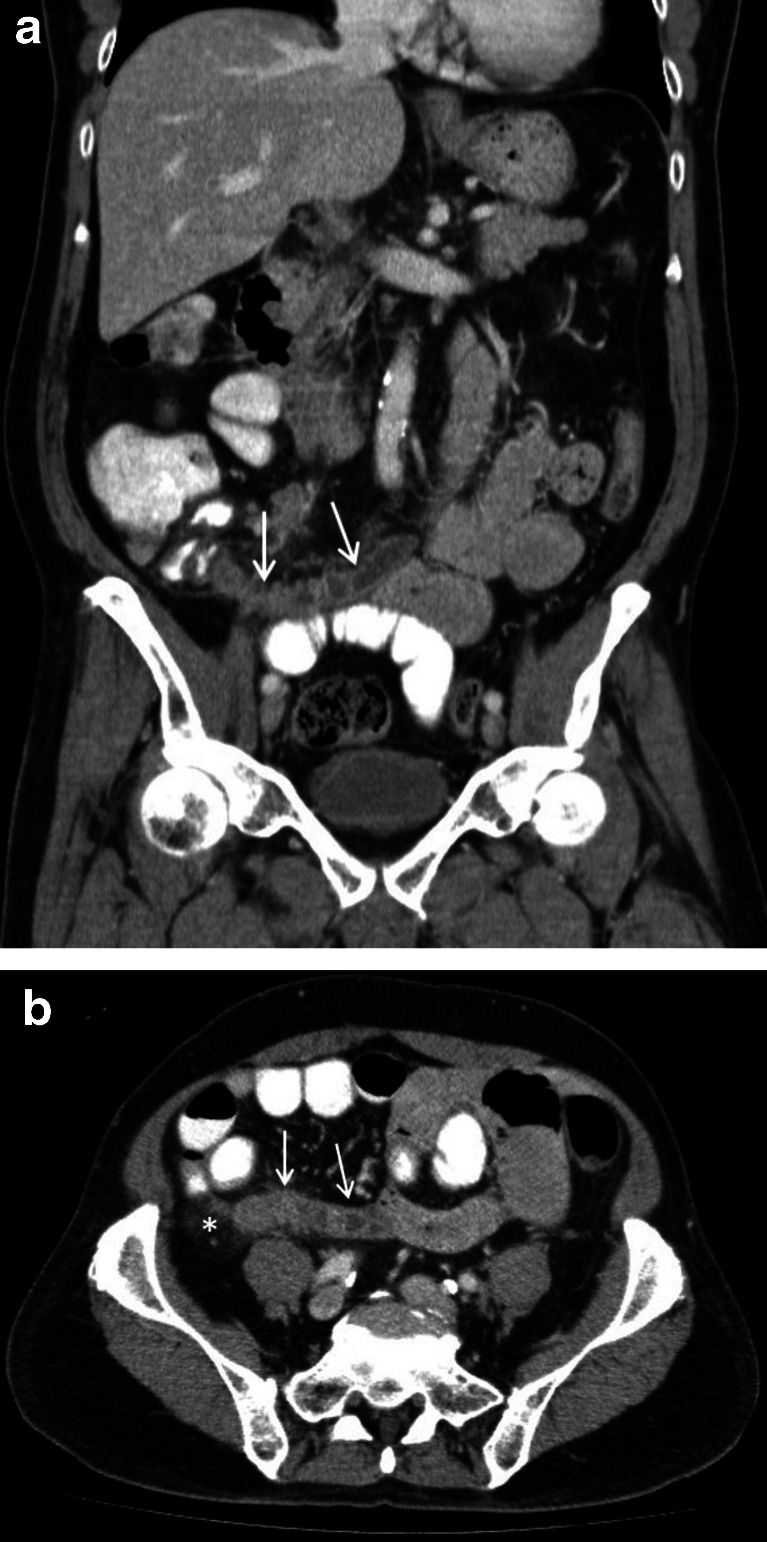
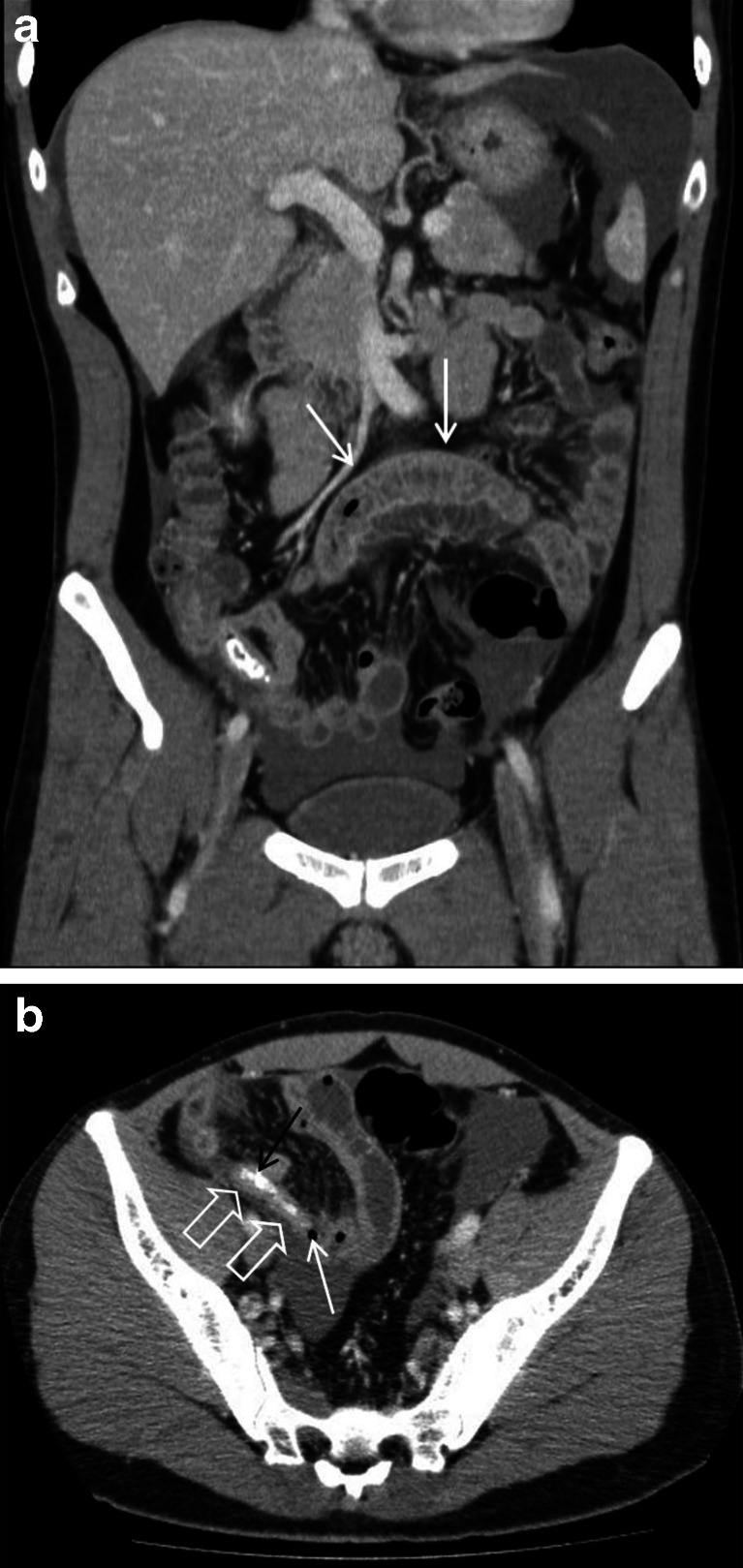
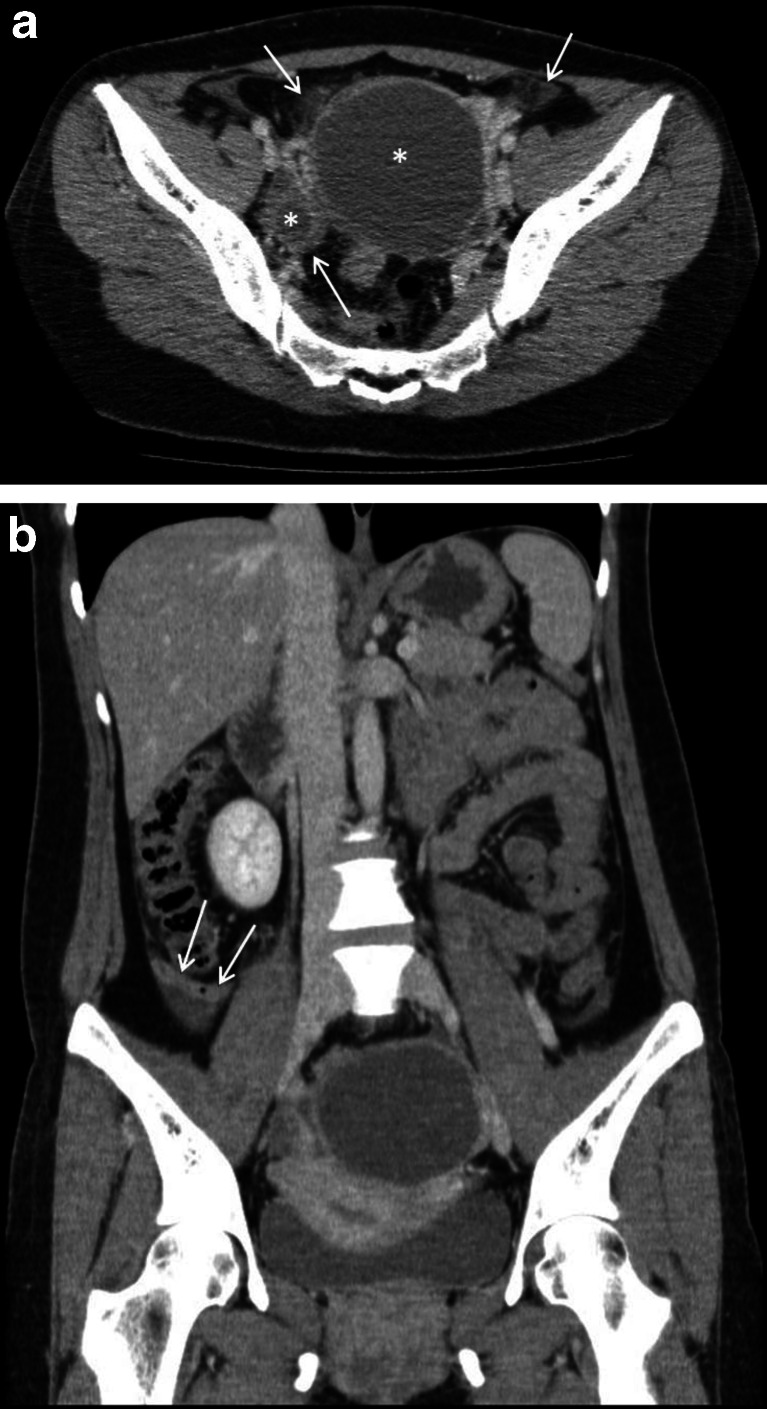
The increasing use of computed tomography (CT) in acute appendicitis makes recognising the radiological hallmarks of the condition and its mimics vital. The differential diagnosis includes both appendiceal and nonappendiceal pathologies. The correlation between pre-appendectomy CT and post-appendectomy histopathology was audited retrospectively. Cases of clinico-histopathological discrepancy underwent blind peer-review, and possible improvements were discussed in the context of the medical literature. A grade for discrepancy was given based on the RADPEER scoring system, and interesting or discrepant cases were examined more closely to identify targets for education. Of the 199 procedures, 4 appendectomies were negative (histologically normal), 182 were positive (primary appendicitis) and 13 were incidental (another primary process caused inflammation). The positive predictive value for pre-appendectomy CT was 91.5 %, and the negative appendectomy rate was 2 %. There were many secondary pathologies, including neoplasia, tuberculosis and endometriosis. Although no CT reports missed a diagnosis that should be made "almost all of the time" and in 96 % of cases, the second, blinded radiologist agreed with the initial assessment, in 3 cases, a missed diagnosis altered clinical management; 2 were "understandable" misses but 1 was not. In five cases, a discrepancy was "understandable" but clinically insignificant. Overall, in comparison to the medical literature, the degree of clinico-histopathological correlation was good. Although identifying areas for improvement was challenging, after a pictorial review of four cases and a discussion of the medical literature, we present our audit results and some valuable learning points for use in the CT assessment of suspected acute appendicitis.
计算机断层扫描(CT)在急性阑尾炎中的应用日益增加,因此识别该病及其类似病症的放射学特征至关重要。鉴别诊断包括阑尾和非阑尾病变。对阑尾切除术前CT与阑尾切除术后组织病理学之间的相关性进行了回顾性审核。对临床组织病理学存在差异的病例进行了盲法同行评审,并结合医学文献讨论了可能的改进措施。根据RADPEER评分系统给出差异等级,并对有趣或存在差异的病例进行更仔细的检查,以确定教育目标。在199例手术中,4例阑尾切除术结果为阴性(组织学正常),182例为阳性(原发性阑尾炎),13例为偶然发现(另一种原发性病变引起炎症)。阑尾切除术前CT的阳性预测值为91.5%,阴性阑尾切除率为2%。存在许多继发性病变,包括肿瘤、结核和子宫内膜异位症。尽管没有CT报告漏诊“几乎所有情况下”都应做出的诊断,并且在96%的病例中,第二位盲法放射科医生同意初始评估,但在3例病例中,漏诊改变了临床管理;2例是“可以理解”的漏诊,但1例不是。在5例病例中,差异是“可以理解”的,但在临床上不显著。总体而言,与医学文献相比,临床组织病理学的相关性程度良好。尽管确定改进领域具有挑战性,但在对4例病例进行图像回顾并讨论医学文献后,我们展示了我们的审核结果以及一些有价值的学习要点,以供在疑似急性阑尾炎的CT评估中使用。