Chawla Anita J, Mytelka Daniel S, McBride Stephan D, Nellesen Dave, Elkins Benjamin R, Ball Daniel E, Kalsekar Anupama, Towse Adrian, Garrison Louis P
Analysis Group, Inc., Menlo Park, CA, USA.
Pharmacoepidemiol Drug Saf. 2014 Mar;23(3):268-77. doi: 10.1002/pds.3559. Epub 2014 Jan 14.
To evaluate the advantages and disadvantages of pre-approval requirements for safety data to detect cardiovascular (CV) risk contained in the December 2008 U.S. Food and Drug Administration (FDA) guidance for developing type 2 diabetes drugs compared with the February 2008 FDA draft guidance from the perspective of diabetes population health.
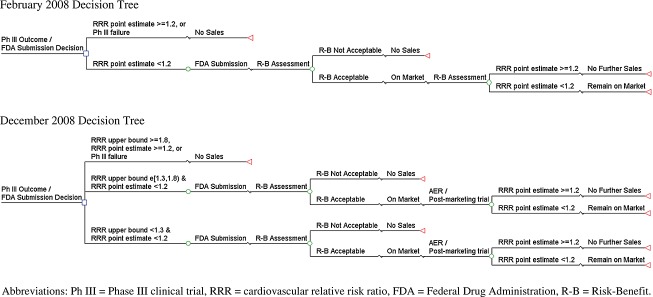
We applied the incremental net health benefit (INHB) framework to quantify the benefits and risks of investigational diabetes drugs using a common survival metric (life-years [LYs]). We constructed a decision analytic model for clinical program development consistent with the requirements of each guidance and simulated diabetes drugs, some of which had elevated CV risk. Assuming constant research budgets, we estimate the impact of increased trial size on drugs investigated. We aggregate treatment benefit and CV risks for each approved drug over a 35-year horizon under each guidance.
The quantitative analysis suggests that the December 2008 guidance adversely impacts diabetes population health. INHB was -1.80 million LYs, attributable to delayed access to diabetes therapies (-0 .18 million LYs) and fewer drugs (-1.64 million LYs), but partially offset by reduced CV risk exposure (0.02 million LYs). Results were robust in sensitivity analyses.
The health outcomes impact of all potential benefits and risks should be evaluated in a common survival measure, including health gain from avoided adverse events, lost health benefits from delayed or for gone efficacious products, and impact of alternative policy approaches. Quantitative analysis of the December 2008 FDA guidance for diabetes therapies indicates that negative impact on patient health will result.
从糖尿病人群健康的角度,评估2008年12月美国食品药品监督管理局(FDA)发布的2型糖尿病药物研发指南中关于安全数据预先批准要求以检测心血管(CV)风险的利弊,与2008年2月FDA的指南草案进行比较。
我们应用增量净健康效益(INHB)框架,使用常见的生存指标(生命年[LYs])来量化研究性糖尿病药物的益处和风险。我们构建了一个与每个指南要求一致的临床项目开发决策分析模型,并模拟了糖尿病药物,其中一些药物具有升高的CV风险。假设研究预算不变,我们估计增加试验规模对所研究药物的影响。我们汇总了在每个指南下,每种获批药物在35年期间的治疗益处和CV风险。
定量分析表明,2008年12月的指南对糖尿病人群健康产生了不利影响。INHB为-180万生命年,这归因于糖尿病治疗药物的获取延迟(-18万生命年)和药物数量减少(-164万生命年),但部分被CV风险暴露的降低(2万生命年)所抵消。敏感性分析结果具有稳健性。
所有潜在益处和风险对健康结果的影响应以共同的生存指标进行评估,包括避免不良事件带来的健康增益、延迟或未能获得有效产品导致的健康益处损失,以及替代政策方法的影响。对2008年12月FDA糖尿病治疗指南的定量分析表明,这将对患者健康产生负面影响。