Departamento de Matemática Aplicada y Estadística e I. O, Universidad del País Vasco UPV/EHU, Leioa, Bizkaia, Spain; Red de Investigación en Servicios de Salud en Enfermedades Crónicas (REDISSEC), Galdakao, Bizkaia, Spain.
Servicio de Neumología, Hospital Galdakao-Usansolo, Galdakao, Bizkaia, Spain; Red de Investigación en Servicios de Salud en Enfermedades Crónicas (REDISSEC), Galdakao, Bizkaia, Spain.
PLoS One. 2014 Jun 3;9(6):e98580. doi: 10.1371/journal.pone.0098580. eCollection 2014.
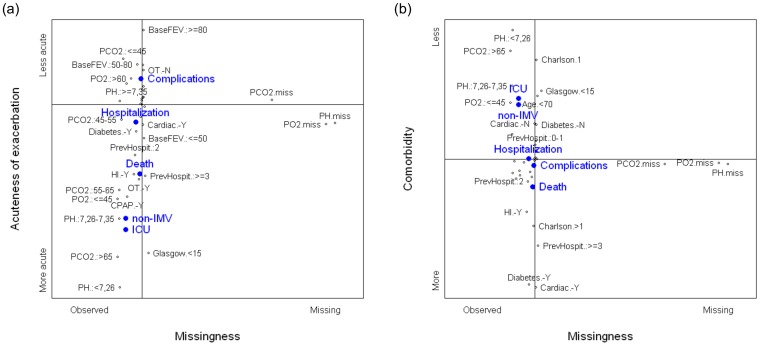
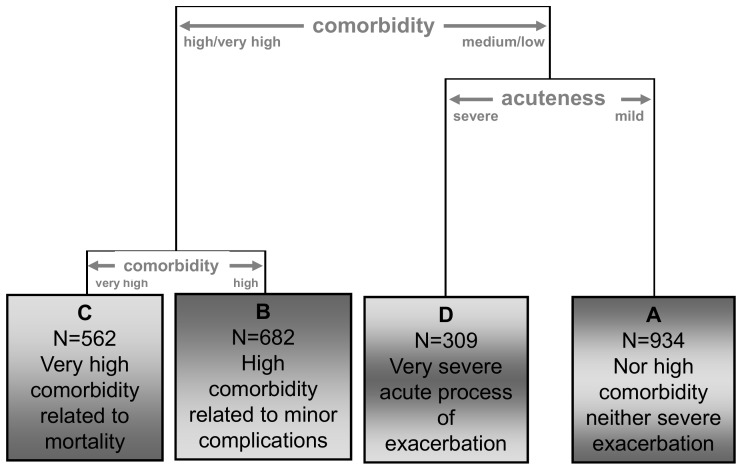
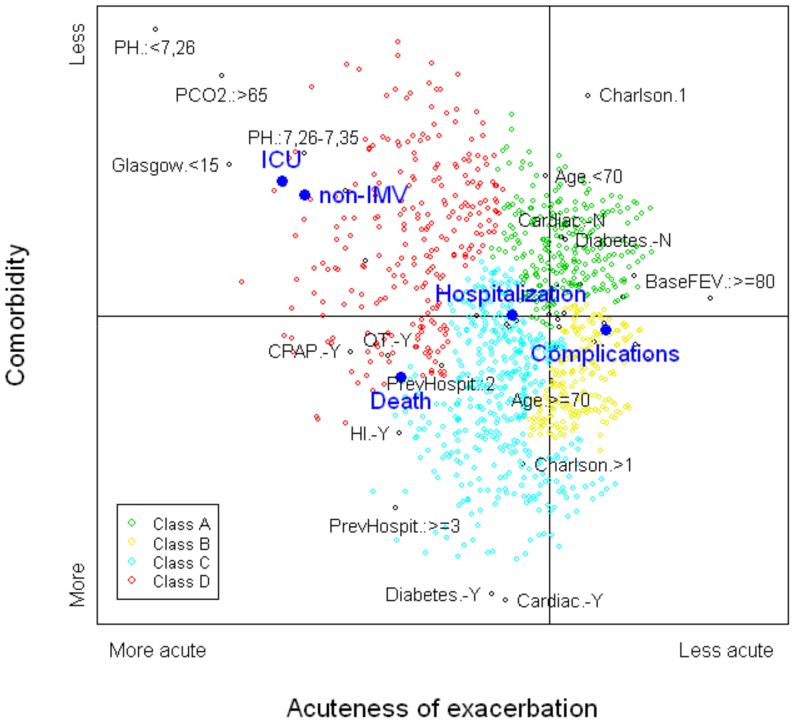
Chronic obstructive pulmonary disease (COPD) is a complex and heterogeneous condition characterized by occasional exacerbations. Identifying clinical subtypes among patients experiencing COPD exacerbations (ECOPD) could help better understand the pathophysiologic mechanisms involved in exacerbations, establish different strategies of treatment, and improve the process of care and patient prognosis. The objective of this study was to identify subtypes of ECOPD patients attending emergency departments using clinical variables and to validate the results using several outcomes. We evaluated data collected as part of the IRYSS-COPD prospective cohort study conducted in 16 hospitals in Spain. Variables collected from ECOPD patients attending one of the emergency departments included arterial blood gases, presence of comorbidities, previous COPD treatment, baseline severity of COPD, and previous hospitalizations for ECOPD. Patient subtypes were identified by combining results from multiple correspondence analysis and cluster analysis. Results were validated using key outcomes of ECOPD evolution. Four ECOPD subtypes were identified based on the severity of the current exacerbation and general health status (largely a function of comorbidities): subtype A (n = 934), neither high comorbidity nor severe exacerbation; subtype B (n = 682), moderate comorbidities; subtype C (n = 562), severe comorbidities related to mortality; and subtype D (n = 309), very severe process of exacerbation, significantly related to mortality and admission to an intensive care unit. Subtype D experienced the highest rate of mortality, admission to an intensive care unit and need for noninvasive mechanical ventilation, followed by subtype C. Subtypes A and B were primarily related to other serious complications. Hospitalization rate was more than 50% for all the subtypes, although significantly higher for subtypes C and D than for subtypes A and B. These results could help identify characteristics to categorize ECOPD patients for more appropriate care, and help test interventions and treatments in subgroups with poor evolution and outcomes.
慢性阻塞性肺疾病(COPD)是一种复杂且异质性的疾病,其特征是偶发加重。在经历 COPD 加重(ECOPD)的患者中识别临床亚型有助于更好地了解加重涉及的病理生理机制,制定不同的治疗策略,并改善护理流程和患者预后。本研究的目的是使用临床变量识别急诊科就诊的 ECOPD 患者的亚型,并使用多种结局验证结果。我们评估了在西班牙 16 家医院进行的前瞻性 IRYSS-COPD 队列研究中收集的数据。从就诊于其中一家急诊科的 ECOPD 患者中收集的变量包括动脉血气、合并症的存在、以前的 COPD 治疗、COPD 基线严重程度和因 ECOPD 住院的次数。通过组合多项对应分析和聚类分析的结果来识别患者亚型。使用 ECOPD 演变的关键结局验证结果。根据当前加重的严重程度和整体健康状况(主要取决于合并症)确定了四种 ECOPD 亚型:亚型 A(n = 934),既没有严重的合并症也没有严重的加重;亚型 B(n = 682),合并症中等;亚型 C(n = 562),严重的与死亡率相关的合并症;和亚型 D(n = 309),非常严重的加重过程,与死亡率和入住重症监护病房密切相关。亚型 D 的死亡率最高,入住重症监护病房和需要无创机械通气的比例最高,其次是亚型 C。亚型 A 和 B 主要与其他严重并发症有关。所有亚型的住院率都超过 50%,但亚型 C 和 D 明显高于亚型 A 和 B。这些结果可以帮助识别特征,对 ECOPD 患者进行分类,以提供更合适的护理,并帮助在预后较差和结局不佳的亚组中测试干预措施和治疗方法。