van Genderen Michel E, Paauwe Jorden, de Jonge Jeroen, van der Valk Ralf J P, Lima Alexandre, Bakker Jan, van Bommel Jasper
Crit Care. 2014 Jun 3;18(3):R114. doi: 10.1186/cc13905.
Altered peripheral perfusion is strongly associated with poor outcome in critically ill patients. We wanted to determine whether repeated assessments of peripheral perfusion during the days following surgery could help to early identify patients that are more likely to develop postoperative complications.
Haemodynamic measurements and peripheral perfusion parameters were collected one day prior to surgery, directly after surgery (D0) and on the first (D1), second (D2) and third (D3) postoperative days. Peripheral perfusion assessment consisted of capillary refill time (CRT), peripheral perfusion index (PPI) and forearm-to-fingertip skin temperature gradient (T(skin-diff)). Generalized linear mixed models were used to predict severe complications within ten days after surgery based on Clavien-Dindo classification.
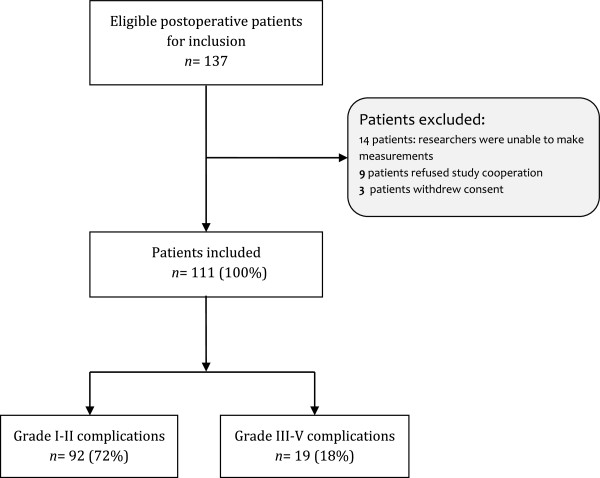
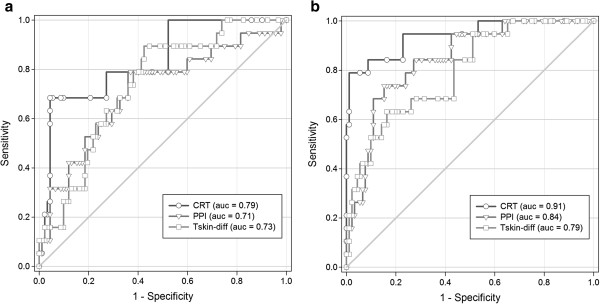
We prospectively followed 137 consecutive patients, from among whom 111 were included in the analysis. Severe complications were observed in 19 patients (17.0%). Postoperatively, peripheral perfusion parameters were significantly altered in patients who subsequently developed severe complications compared to those who did not, and these parameters persisted over time. CRT was altered at D0, and PPI and T(skin-diff) were altered on D1 and D2, respectively. Among the different peripheral perfusion parameters, the diagnostic accuracy in predicting severe postoperative complications was highest for CRT on D2 (area under the receiver operating characteristic curve = 0.91 (95% confidence interval (CI) = 0.83 to 0.92)) with a sensitivity of 0.79 (95% CI = 0.54 to 0.94) and a specificity of 0.93 (95% CI = 0.86 to 0.97). Generalized mixed-model analysis demonstrated that abnormal peripheral perfusion on D2 and D3 was an independent predictor of severe postoperative complications (D2 odds ratio (OR) = 8.4, 95% CI = 2.7 to 25.9; D2 OR = 6.4, 95% CI = 2.1 to 19.6).
In a group of patients assessed following major abdominal surgery, peripheral perfusion alterations were associated with the development of severe complications independently of systemic haemodynamics. Further research is needed to confirm these findings and to explore in more detail the effects of peripheral perfusion-targeted resuscitation following major abdominal surgery.
外周灌注改变与危重症患者的不良预后密切相关。我们想确定术后数天内反复评估外周灌注是否有助于早期识别更易发生术后并发症的患者。
在手术前一天、手术刚结束时(D0)以及术后第一天(D1)、第二天(D2)和第三天(D3)收集血流动力学测量值和外周灌注参数。外周灌注评估包括毛细血管再充盈时间(CRT)、外周灌注指数(PPI)和前臂至指尖皮肤温度梯度(T(skin-diff))。基于Clavien-Dindo分类,使用广义线性混合模型预测术后十天内的严重并发症。
我们前瞻性地跟踪了137例连续患者,其中111例纳入分析。19例患者(17.0%)出现严重并发症。术后,与未发生严重并发症的患者相比,随后发生严重并发症的患者外周灌注参数有显著改变,且这些参数随时间持续存在。CRT在D0时改变,PPI和T(skin-diff)分别在D1和D2时改变。在不同的外周灌注参数中,D2时CRT预测严重术后并发症的诊断准确性最高(受试者工作特征曲线下面积 = 0.91(95%置信区间(CI) = 0.83至0.92)),敏感性为0.79(95%CI = 0.54至0.94),特异性为0.93(95%CI = 0.86至0.97)。广义混合模型分析表明,D2和D3时外周灌注异常是严重术后并发症的独立预测因素(D2比值比(OR) = 8.4,95%CI = 2.7至25.9;D3 OR = 6.4,95%CI = 2.1至19.6)。
在一组接受大腹部手术后评估的患者中,外周灌注改变与严重并发症的发生相关,且独立于全身血流动力学。需要进一步研究来证实这些发现,并更详细地探讨大腹部手术后外周灌注靶向复苏的效果。