Coplan Jeremy D, Gopinath Srinath, Abdallah Chadi G, Berry Benjamin R
Division of Neuropsychopharmacology, Department of Psychiatry and Behavioral Science, State University of New York Downstate Medical Center , Brooklyn, NY , USA.
Department of Psychiatry, Yale School of Medicine , New Haven, CT , USA ; Clinical Neuroscience Division, National Center for PTSD , West Haven, CT , USA.
Front Behav Neurosci. 2014 May 20;8:189. doi: 10.3389/fnbeh.2014.00189. eCollection 2014.
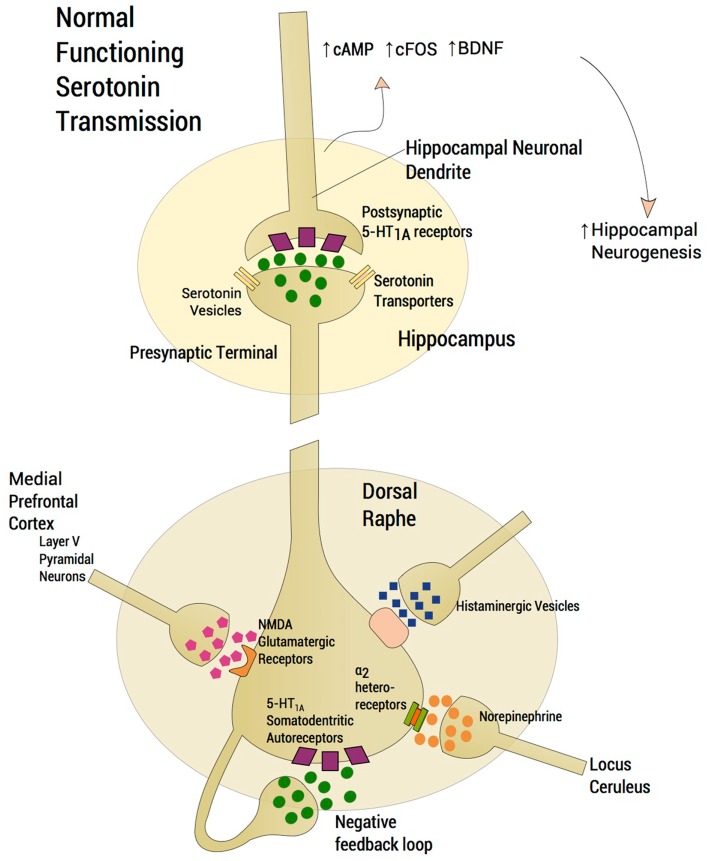
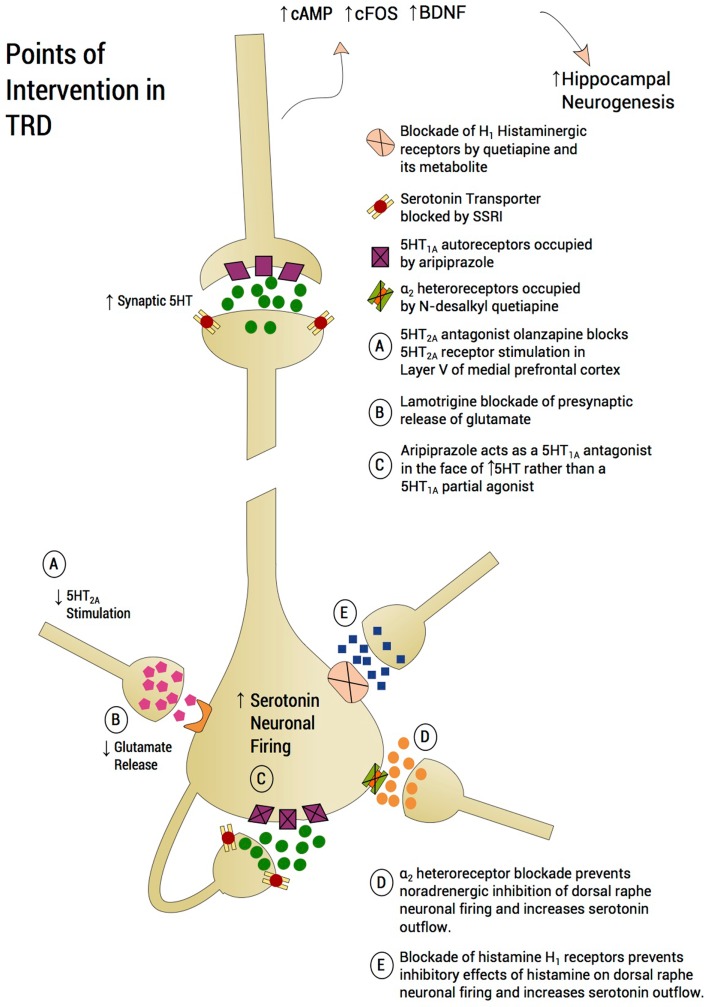
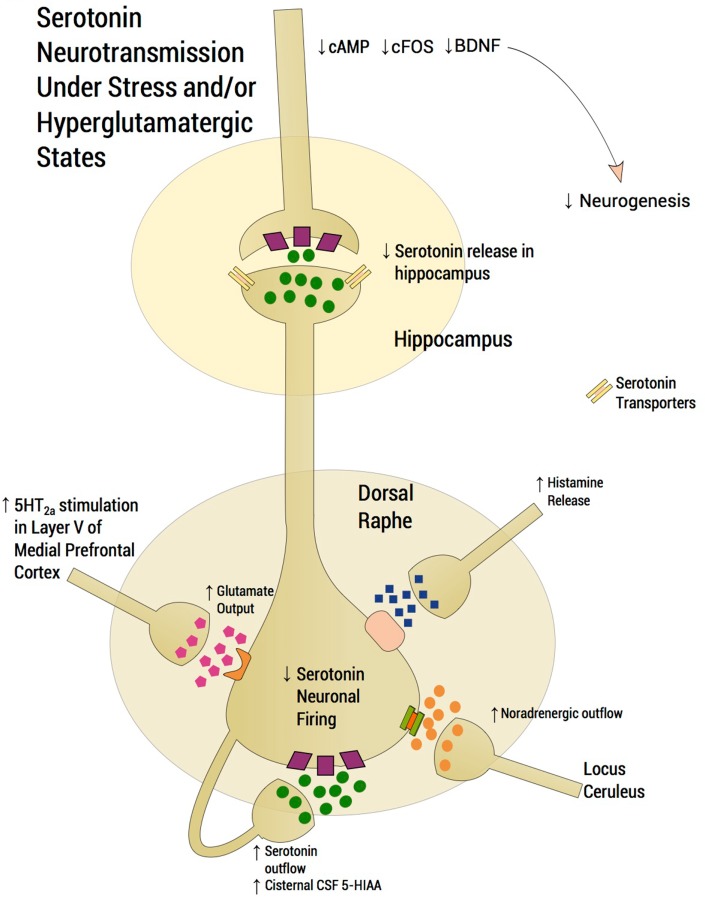
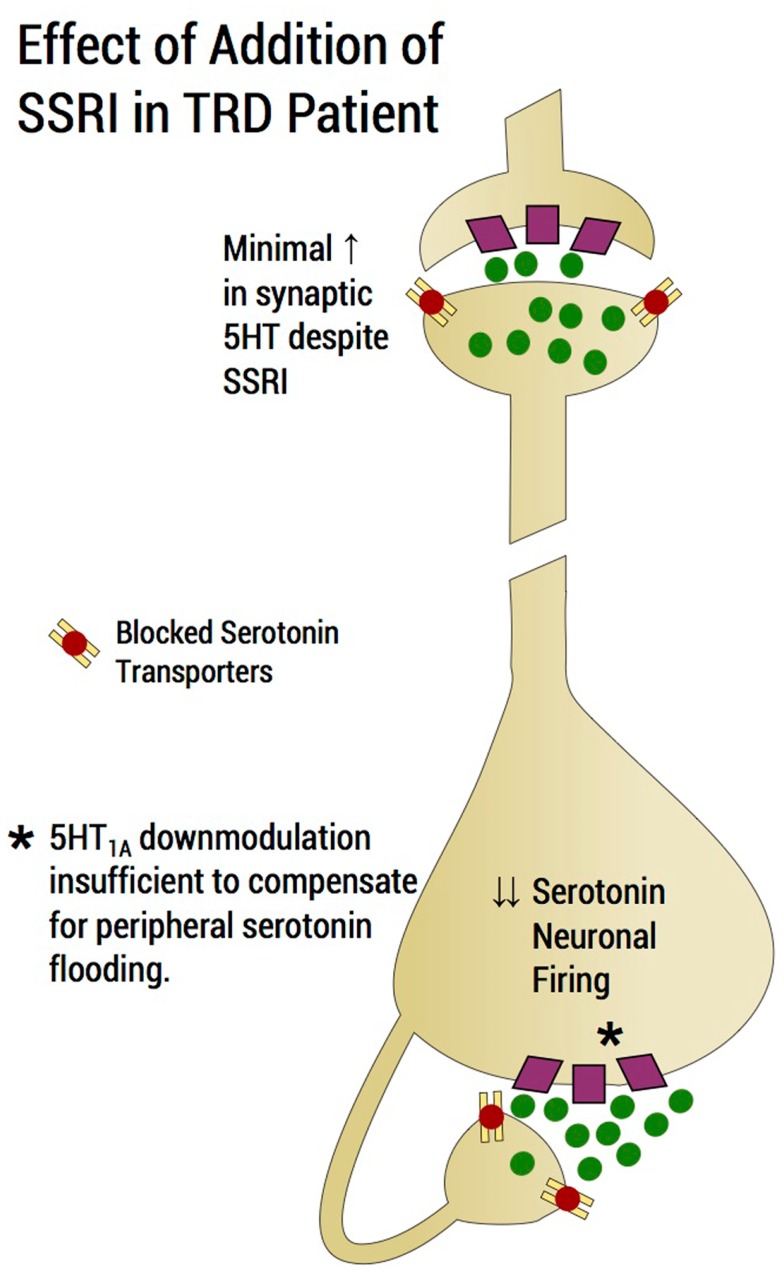
First-line treatment of major depression includes administration of a selective serotonin reuptake inhibitor (SSRI), yet studies suggest that remission rates following two trials of an SSRI are <50%. The authors examine the putative biological substrates underlying "treatment resistant depression (TRD)" with the goal of elucidating novel rationales to treat TRD. We look at relevant articles from the preclinical and clinical literature combined with clinical exposure to TRD patients. A major focus was to outline pathophysiological mechanisms whereby the serotonin system becomes impervious to the desired enhancement of serotonin neurotransmission by SSRIs. A complementary focus was to dissect neurotransmitter systems, which serve to inhibit the dorsal raphe. We propose, based on a body of translational studies, TRD may not represent a simple serotonin deficit state but rather an excess of midbrain peri-raphe serotonin and subsequent deficit at key fronto-limbic projection sites, with ultimate compromise in serotonin-mediated neuroplasticity. Glutamate, serotonin, noradrenaline, and histamine are activated by stress and exert an inhibitory effect on serotonin outflow, in part by "flooding" 5-HT1A autoreceptors by serotonin itself. Certain factors putatively exacerbate this scenario - presence of the short arm of the serotonin transporter gene, early-life adversity and comorbid bipolar disorder - each of which has been associated with SSRI-treatment resistance. By utilizing an incremental approach, we provide a system for treating the TRD patient based on a strategy of rescuing serotonin neurotransmission from a state of SSRI-induced dorsal raphe stasis. This calls for "stacked" interventions, with an SSRI base, targeting, if necessary, the glutamatergic, serotonergic, noradrenergic, and histaminergic systems, thereby successively eliminating the inhibitory effects each are capable of exerting on serotonin neurons. Future studies are recommended to test this biologically based approach for treatment of TRD.
重度抑郁症的一线治疗包括给予选择性5-羟色胺再摄取抑制剂(SSRI),然而研究表明,经过两次SSRI试验后的缓解率<50%。作者研究了“难治性抑郁症(TRD)”潜在的生物学基础,目的是阐明治疗TRD的新原理。我们查阅了临床前和临床文献中的相关文章,并结合对TRD患者的临床接触情况进行分析。一个主要重点是概述5-羟色胺系统对SSRI所期望的5-羟色胺神经传递增强作用变得无反应的病理生理机制。一个补充重点是剖析用于抑制中缝背核的神经递质系统。基于一系列转化研究,我们提出,TRD可能并不代表简单的5-羟色胺缺乏状态,而是中脑缝周5-羟色胺过多以及关键额-边缘投射部位随后出现缺乏,最终导致5-羟色胺介导的神经可塑性受损。谷氨酸、5-羟色胺、去甲肾上腺素和组胺会因应激而被激活,并对5-羟色胺流出产生抑制作用,部分原因是5-羟色胺自身“充斥”5-HT1A自受体。某些因素可能会加剧这种情况——5-羟色胺转运体基因短臂的存在、早年逆境和双相情感障碍共病——每一种都与SSRI治疗抵抗有关。通过采用渐进式方法,我们提供了一个基于从SSRI诱导的中缝背核停滞状态挽救5-羟色胺神经传递策略的TRD患者治疗系统。这需要“叠加”干预措施,以SSRI为基础,必要时针对谷氨酸能、5-羟色胺能、去甲肾上腺素能和组胺能系统,从而依次消除它们各自对5-羟色胺神经元施加的抑制作用。建议未来的研究测试这种基于生物学的TRD治疗方法。