Department of General and Transplant Surgery, Ruprecht-Karls University, Heidelberg, Germany.
PLoS One. 2014 Jun 6;9(6):e98782. doi: 10.1371/journal.pone.0098782. eCollection 2014.
Liver transplantation is the only curative treatment for end-stage liver disease. While waiting list mortality can be predicted by the MELD-score, reliable scoring systems for the postoperative period do not exist. This study's objective was to identify risk factors that contribute to postoperative mortality.
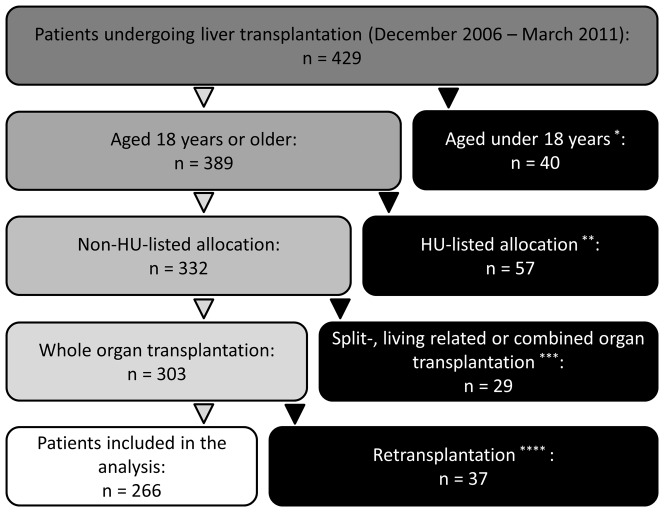
Between December 2006 and March 2011, 429 patients underwent liver transplantation in our department. Risk factors for postoperative mortality in 266 consecutive liver transplantations were identified using univariate and multivariate analyses. Patients who were <18 years, HU-listings, and split-, living related, combined or re-transplantations were excluded from the analysis. The correlation between number of risk factors and mortality was analyzed.
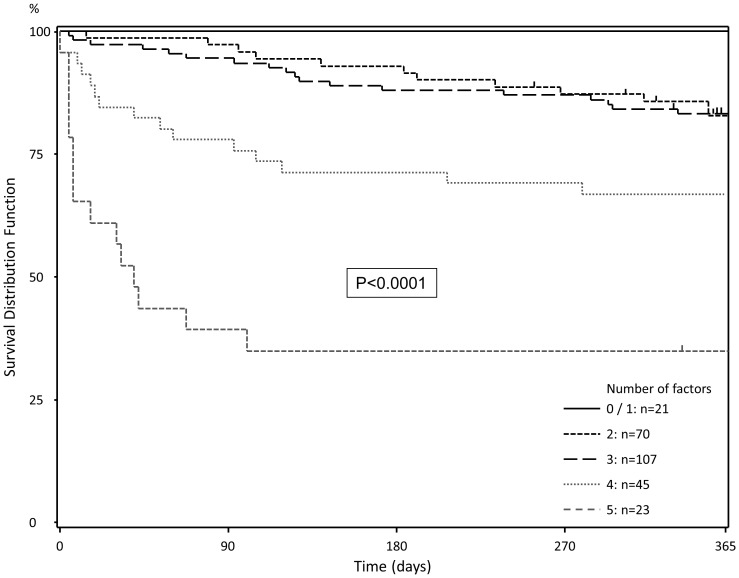
A labMELD ≥20, female sex, coronary heart disease, donor risk index >1.5 and donor Na+>145 mmol/L were identified to be independent predictive factors for postoperative mortality. With increasing number of these risk-factors, postoperative 90-day and 1-year mortality increased (0-1: 0 and 0%; 2: 2.9 and 17.4%; 3: 5.6 and 16.8%; 4: 22.2 and 33.3%; 5-6: 60.9 and 66.2%).
In this analysis, a simple score was derived that adequately identified patients at risk after liver transplantation. Opening a discussion on the inclusion of these parameters in the process of organ allocation may be a worthwhile venture.
肝移植是治疗终末期肝病的唯一根治方法。虽然 MELD 评分可以预测等待名单上的死亡率,但术后没有可靠的评分系统。本研究的目的是确定导致术后死亡的危险因素。
2006 年 12 月至 2011 年 3 月,我院共进行了 429 例肝移植手术。本研究采用单因素和多因素分析,确定了 266 例连续肝移植患者术后死亡的危险因素。本研究排除了年龄<18 岁、HU 名单、劈裂、活体相关、联合或再次移植的患者。分析了风险因素的数量与死亡率之间的相关性。
实验室 MELD 评分≥20、女性、冠心病、供体风险指数>1.5 和供体 Na+>145mmol/L 被确定为术后死亡的独立预测因素。随着这些危险因素数量的增加,术后 90 天和 1 年的死亡率也随之增加(0-1:0%和 0%;2:2.9%和 17.4%;3:5.6%和 16.8%;4:22.2%和 33.3%;5-6:60.9%和 66.2%)。
在本分析中,得出了一个简单的评分,可以充分识别肝移植后有风险的患者。在器官分配过程中讨论纳入这些参数可能是值得的。