Waheed Salman, Azad Nilofer, Waheed Sehrish, Yeh Hsin-Chieh
Department of Medicine, The Johns Hopkins University, Baltimore, Maryland, USA; Department of Epidemiology, The Johns Hopkins University, Baltimore, Maryland, USA.
J Gastroenterol Hepatol. 2014 Dec;29(12):1963-8. doi: 10.1111/jgh.12637.
To investigate whether pre-existing diabetes modifies racial disparities in colorectal cancer (CRC) survival.
We analyzed prospective data from 16 977 patients (age ≥ 67 years) with CRC from the Surveillance Epidemiology and End Results (SEER)-Medicare database. SEER registries included data on demographics, tumor characteristics, and treatment. Medicare claims were used to define pre-existing diabetes and comorbid conditions. Mortality was confirmed in both sources.
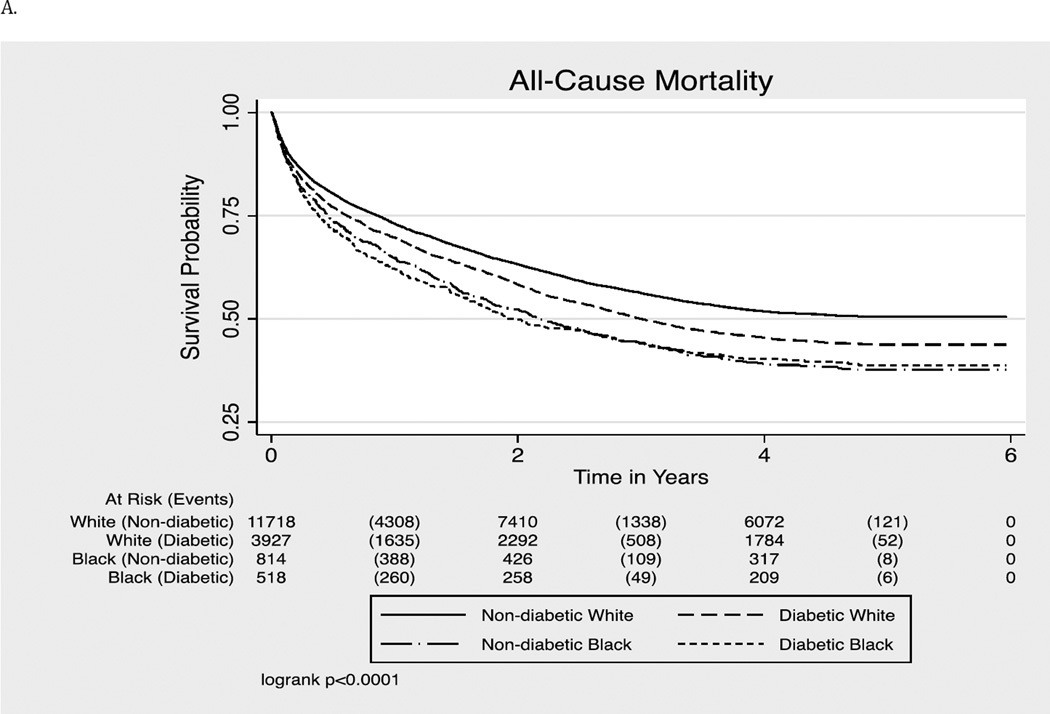
At baseline, 1332 (8%) were African Americans and 26% had diabetes (39% in blacks; 25% in whites). From 2000 to 2005, more than half of the participants died (n = 8782, 52%). This included 820 (62%) deaths (23.8 per 100 person-years) among blacks, and 7962 (51%) deaths (16.6 per 100 person-years) among whites. Among older adults with diabetes, blacks had significantly higher risk of all-cause and CRC mortality after adjustments for demographic characteristics (hazard ratio [HR], 95% confidence interval [CI]: 1.21 [1.08-1.37] and 1.21 [1.03-1.42]), respectively, but these associations attenuated to null after additional adjustments for cancer stage and grade. Among adults without diabetes, the risk of all-cause mortality (HR [95% CI]: 1.14 [1.04-1.25]) and CRC mortality (HR [95% CI]: 1.21 [1.08-1.36]) remained higher in blacks than whites in fully adjusted models that included demographic variables, cancer stage, grade, treatments, and comorbidities.
Among older adults with CRC, diabetes is an effect modifier on the relationship between race and mortality. Racial disparities in survival were explained by demographics, cancer stage, and grade in patients with diabetes.
探讨既往糖尿病是否会改变结直肠癌(CRC)生存方面的种族差异。
我们分析了来自监测、流行病学和最终结果(SEER)-医疗保险数据库中16977例年龄≥67岁的CRC患者的前瞻性数据。SEER登记处包含人口统计学、肿瘤特征和治疗的数据。医疗保险理赔数据用于定义既往糖尿病和合并症。两个数据源均确认了死亡率。
基线时,1332例(8%)为非裔美国人,26%患有糖尿病(黑人中为39%;白人中为25%)。2000年至2005年期间,超过一半的参与者死亡(n = 8782,52%)。这包括黑人中820例(62%)死亡(每100人年23.8例),白人中7962例(51%)死亡(每100人年16.6例)。在患有糖尿病的老年人中,调整人口统计学特征后,黑人全因死亡率和CRC死亡率的风险显著更高(风险比[HR],95%置信区间[CI]:分别为1.21[1.08 - 1.37]和1.21[1.03 - 1.42]),但在进一步调整癌症分期和分级后,这些关联减弱至无统计学意义。在无糖尿病的成年人中,在纳入人口统计学变量、癌症分期、分级、治疗和合并症的完全调整模型中,黑人的全因死亡率(HR[95%CI]:1.14[1.04 - 1.25])和CRC死亡率(HR[95%CI]:1.21[1.08 - 1.36])仍高于白人。
在患有CRC的老年人中,糖尿病是种族与死亡率关系的效应修饰因素。糖尿病患者生存方面的种族差异可由人口统计学、癌症分期和分级来解释。