Hulzebos Christian V, Dijk Peter H, van Imhoff Deirdre E, Bos Arend F, Lopriore Enrico, Offringa Martin, Ruiter Selma A J, van Braeckel Koen N J A, Krabbe Paul F M, Quik Elise H, van Toledo-Eppinga Letty, Nuytemans Debbie H G M, van Wassenaer-Leemhuis Aleid G, Benders Manon J N, Korbeeck-van Hof Karen K M, van Lingen Richard A, Groot Jebbink Liesbeth J M, Liem Djien, Mansvelt Petri, Buijs Jan, Govaert Paul, van Vliet Ineke, Mulder Twan L M, Wolfs Cecile, Fetter Willem P F, Laarman Celeste
Department of Neonatology, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, The Netherlands.
Division of Neonatology, Department of Pediatrics, Leiden University Medical Center, Leiden, The Netherlands.
PLoS One. 2014 Jun 13;9(6):e99466. doi: 10.1371/journal.pone.0099466. eCollection 2014.
High bilirubin/albumin (B/A) ratios increase the risk of bilirubin neurotoxicity. The B/A ratio may be a valuable measure, in addition to the total serum bilirubin (TSB), in the management of hyperbilirubinemia. We aimed to assess whether the additional use of B/A ratios in the management of hyperbilirubinemia in preterm infants improved neurodevelopmental outcome.
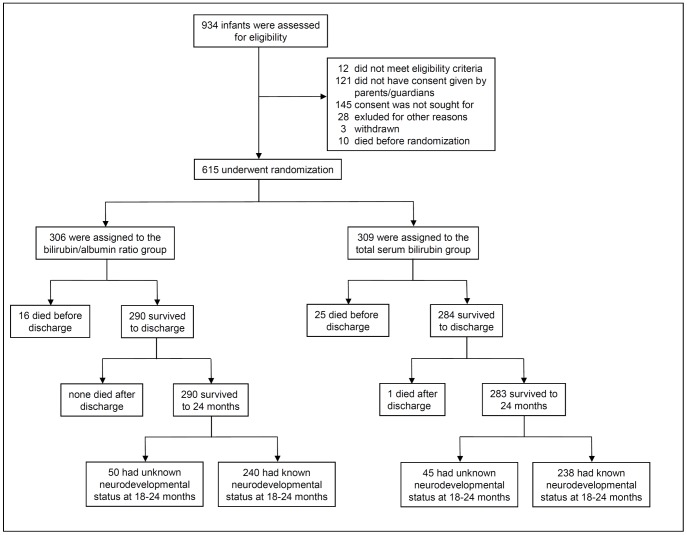
In a prospective, randomized controlled trial, 615 preterm infants of 32 weeks' gestation or less were randomly assigned to treatment based on either B/A ratio and TSB thresholds (consensus-based), whichever threshold was crossed first, or on the TSB thresholds only. The primary outcome was neurodevelopment at 18 to 24 months' corrected age as assessed with the Bayley Scales of Infant Development III by investigators unaware of treatment allocation. Secondary outcomes included complications of preterm birth and death.
Composite motor (100 ± 13 vs. 101 ± 12) and cognitive (101 ± 12 vs. 101 ± 11) scores did not differ between the B/A ratio and TSB groups. Demographic characteristics, maximal TSB levels, B/A ratios, and other secondary outcomes were similar. The rates of death and/or severe neurodevelopmental impairment for the B/A ratio versus TSB groups were 15.4% versus 15.5% (P = 1.0) and 2.8% versus 1.4% (P = 0.62) for birth weights ≤ 1000 g and 1.8% versus 5.8% (P = 0.03) and 4.1% versus 2.0% (P = 0.26) for birth weights of >1000 g.
The additional use of B/A ratio in the management of hyperbilirubinemia in preterm infants did not improve their neurodevelopmental outcome.
Controlled-Trials.com ISRCTN74465643.
高胆红素/白蛋白(B/A)比值会增加胆红素神经毒性的风险。除总血清胆红素(TSB)外,B/A比值可能是管理高胆红素血症的一项重要指标。我们旨在评估在早产儿高胆红素血症管理中额外使用B/A比值是否能改善神经发育结局。
在一项前瞻性随机对照试验中,615名孕周小于或等于32周的早产儿被随机分配接受基于B/A比值和TSB阈值(基于共识)的治疗,以先达到的阈值为准,或仅基于TSB阈值进行治疗。主要结局是在18至24个月矫正年龄时的神经发育情况,由不知道治疗分配情况的研究人员使用贝利婴幼儿发展量表第三版进行评估。次要结局包括早产并发症和死亡。
B/A比值组和TSB组的综合运动(100±13 vs. 101±12)和认知(101±12 vs. 101±11)得分没有差异。人口统计学特征、最高TSB水平、B/A比值和其他次要结局相似。出生体重≤1000g时,B/A比值组与TSB组的死亡和/或严重神经发育障碍发生率分别为15.4%对15.5%(P = 1.0)和2.8%对1.4%(P = 0.62);出生体重>1000g时,分别为1.8%对5.8%(P = 0.03)和4.1%对2.0%(P = 0.26)。
在早产儿高胆红素血症管理中额外使用B/A比值并不能改善其神经发育结局。
Controlled-Trials.com ISRCTN74465643。