Ichikawa Tomoaki, Sano Katsuhiro, Morisaka Hiroyuki
Department of Radiology, University of Yamanashi, Yamanashi, Japan.
Liver Cancer. 2014 May;3(2):97-107. doi: 10.1159/000343865.
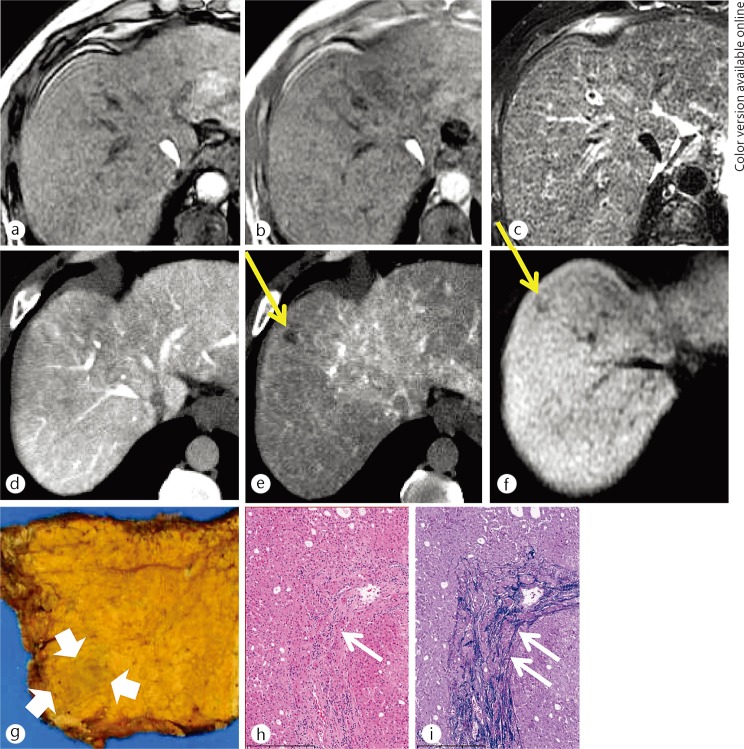
After much debate, the International Consensus Group for Hepatocellular Neoplasia (ICGHN) has recently arrived at a conclusion regarding the pathological criteria for early hepatocellular carcinoma (HCC). They have stated that stromal invasion should be recognized as the most important pathological finding for precisely diagnosing and differentiating early HCC from dysplastic nodules (DN).
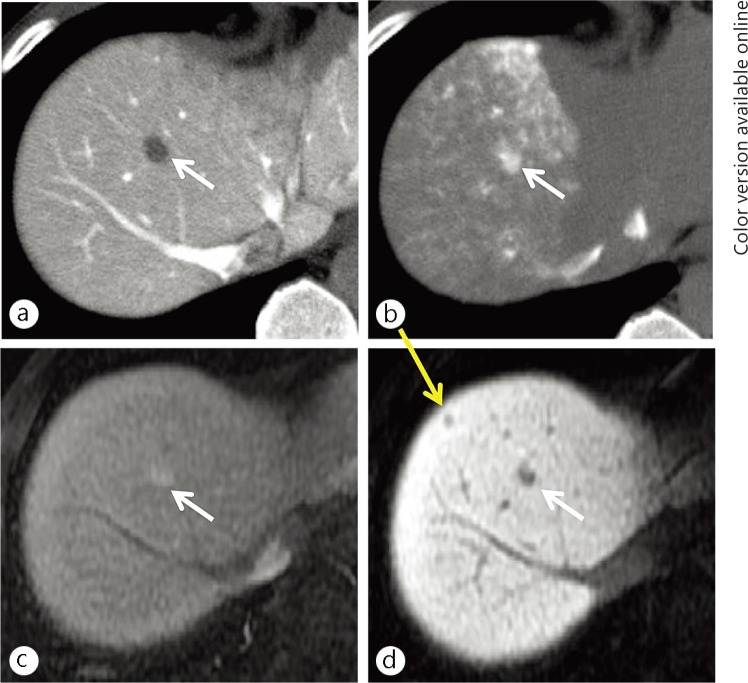
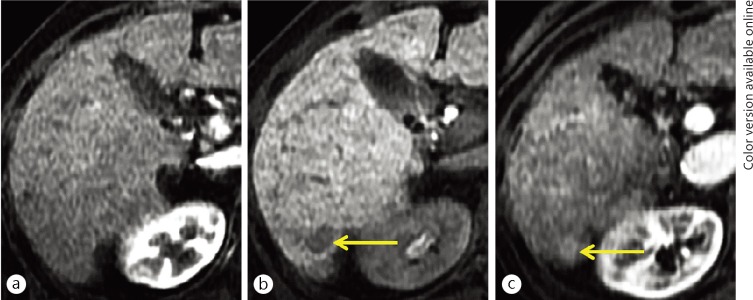
We conducted a review of the imaging findings from multi-imaging modalities of early HCC cases diagnosed according to the pathological criteria of the ICGHN. The multi-imaging modalities included gadoxetic acid (Gd-EOB-DTPA) enhanced magnetic resonance imaging (MRI), abbreviated as EOB-MRI, contrast-enhanced CT (CE-CT), CT during arterioportography (CTAP), and CT during hepatic arteriography (CTHA). It has been shown that EOB-MRI is the only imaging modality that has sufficient resolution for the detection and classification of early HCC.
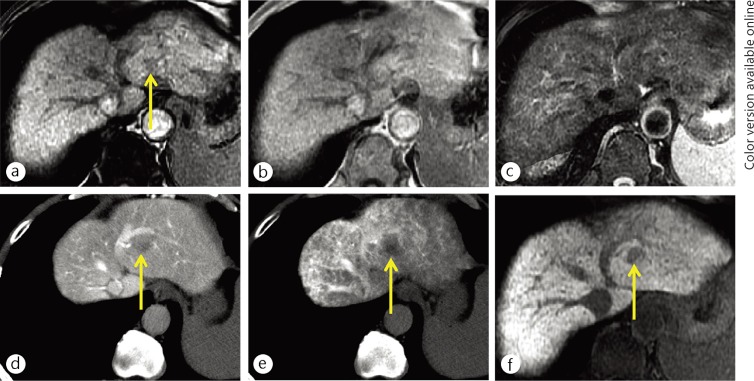
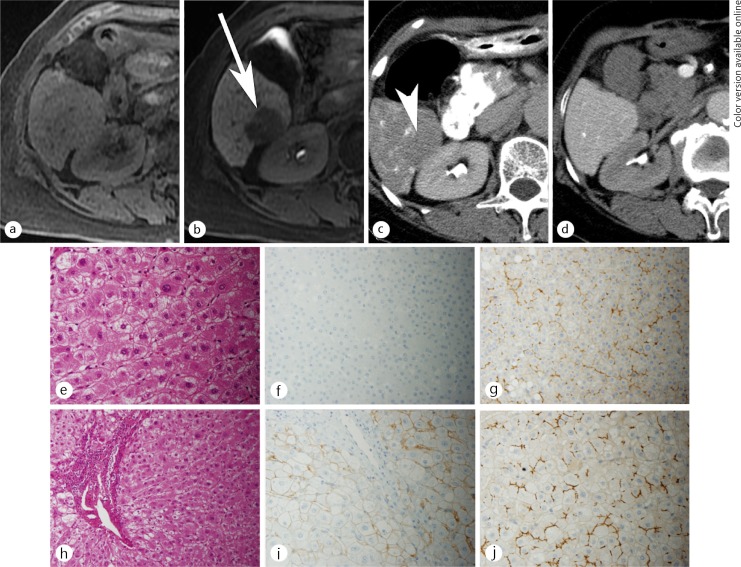
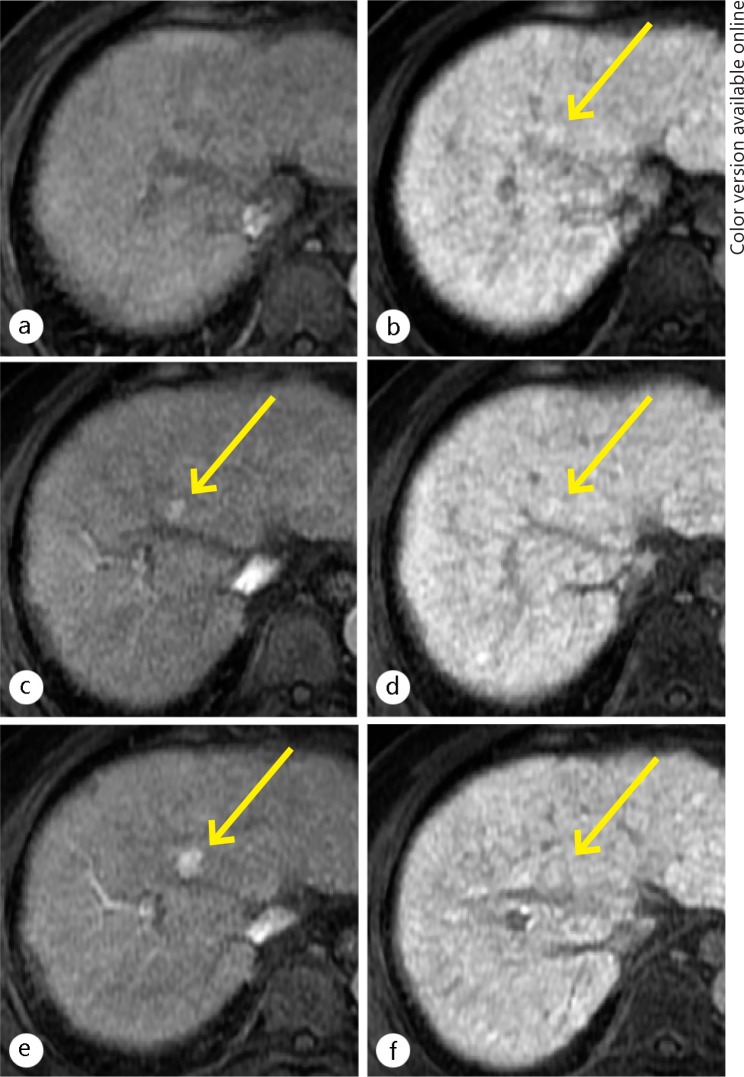
The most significant imaging feature for diagnosing early HCC was hypointensity on hepatobiliary-phase (HP) images of EOB-MRI; all of the cases of early HCC that were detected on HP images of EOB-MRI showed hypointensity, while all of the images of DN showed isointensity or hyperintensity compared with the liver parenchyma. The results of the diagnostic performance analysis showed that EOB-MRI had excellent sensitivity (97%) for detecting early HCC and outstanding specificity (100%) for distinguishing early HCC from DN.
Considering the results from imaging-pathologic correlations and follow-up studies indicating that many early-stage hepatocellular nodules showing hypointensity on HP images of EOB-MRI tend to develop hypervascularization during a relatively short follow-up period, it is beginning to be accepted that such nodules may be treated as early HCC. However, hepatologists and radiologists should also recognize that some cases of early HCC may show isointensity or hyperintensity on HP images of EOB-MRI, making it impossible to differentiate early HCC from DN, although the low prevalence of such nodules may be unlikely to affect the generally accepted follow-up protocols for cirrhotic patients. Our results and other recent reports have indicated that signal-intensity patterns on HP images of EOB-MRI for DN and early HCC directly correlate with the degree of expression of the organic anion transporting polypeptide (OATP) 1B3 in the nodules. Thus, the diagnostic performance of pathological analyses for early HCC cases may be dramatically improved, nearly up to that of EOB-MRI, by incorporating an OATP1B3 staining method.
经过大量讨论,国际肝细胞肿瘤共识小组(ICGHN)最近就早期肝细胞癌(HCC)的病理标准达成了结论。他们指出,间质浸润应被视为精确诊断早期HCC并将其与发育异常结节(DN)区分开来的最重要病理发现。
我们回顾了根据ICGHN病理标准诊断的早期HCC病例的多种影像学检查结果。这些多种影像学检查包括钆塞酸二钠(Gd-EOB-DTPA)增强磁共振成像(MRI),简称为EOB-MRI、对比增强CT(CE-CT)、动脉门静脉造影CT(CTAP)和肝动脉造影CT(CTHA)。已表明EOB-MRI是唯一对早期HCC检测和分类具有足够分辨率的影像学检查。
诊断早期HCC的最显著影像学特征是EOB-MRI肝胆期(HP)图像上的低信号;在EOB-MRI的HP图像上检测到的所有早期HCC病例均显示低信号,而与肝实质相比,DN的所有图像均显示等信号或高信号。诊断性能分析结果表明,EOB-MRI对早期HCC检测具有出色的敏感性(97%),对区分早期HCC与DN具有出色的特异性(100%)。
考虑到影像学-病理相关性及随访研究结果表明,许多在EOB-MRI的HP图像上显示低信号的早期肝细胞结节在相对较短的随访期内倾向于发展为血管增多,开始有人认为此类结节可被视为早期HCC进行治疗。然而,肝病学家和放射科医生也应认识到,一些早期HCC病例在EOB-MRI的HP图像上可能显示等信号或高信号,从而无法将早期HCC与DN区分开来,尽管此类结节的低发生率可能不太可能影响普遍接受的肝硬化患者随访方案。我们的结果及其他近期报告表明,DN和早期HCC在EOB-MRI的HP图像上的信号强度模式与结节中有机阴离子转运多肽(OATP)1B3的表达程度直接相关。因此,通过纳入OATP1B3染色方法,早期HCC病例病理分析的诊断性能可能会显著提高,几乎可达到EOB-MRI的水平。