Perinatal Epidemiology Research Unit, Aarhus University Hospital, Brendstrupgaardsvej 100, Aarhus N 8200, Denmark.
BMC Pediatr. 2014 Jun 19;14:155. doi: 10.1186/1471-2431-14-155.
The INtubation-SURfactant-Extubation (INSURE) is a procedure that is increasingly being used to treat the respiratory distress syndrome in preterm infants. The objective of this study was to identify predictors for an unsuccessful INSURE procedure.
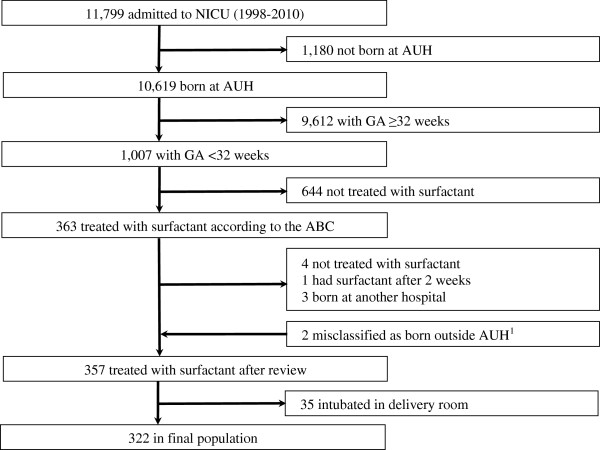
The neonates included were less than 32 weeks' gestation, treated with surfactant in the neonatal intensive care unit, and born 1998-2010. INSURE was defined as surfactant administration during intubation for less than 2 hours without the need for mechanical ventilation. INSURE success was defined as no re-intubation within 72 hours after INSURE, and INSURE failure was defined as re-intubation within 72 hours after INSURE. An unsuccessful INSURE procedure was either INSURE failure or mechanical ventilation for more than 24 hours immediately after surfactant administration. All predictors were defined a priori and were present before surfactant administration. Multivariate logistic regression was performed.
In total, 322 neonates were included: 31% (n = 100) had INSURE success, 10% (n = 33) had INSURE failure, 49% (n = 158) needed mechanical ventilation for more than 24 hours, and the remaining 10% (n = 31) needed mechanical ventilation for less than 24 hours. Predictors for INSURE failure were low gestational age and hemoglobin below 8.5 mmol/l. Predictors for mechanical ventilation for more than 24 hours were low gestational age, Apgar at 5 minutes below 7, oxygen need above 50%, CO2 pressure above 7 kPa (~53 mmHg), pH below 7.3, lactate above 2.5 mmol/l, need for inotropes, and surfactant administration shortly after birth, whereas preeclampsia reduced the risk.
We identified specific predictors associated with an unsuccessful INSURE procedure. Keeping high-risk neonates with one or several predictors intubated and treated with mechanical ventilation after surfactant may prevent a re-intubation procedure.
INtubation-SURfactant-Extubation(INSURE)是一种越来越多地用于治疗早产儿呼吸窘迫综合征的方法。本研究的目的是确定 INSURE 程序不成功的预测因素。
纳入的新生儿胎龄小于 32 周,在新生儿重症监护病房接受表面活性剂治疗,出生于 1998 年至 2010 年。INSURE 定义为在插管期间给予表面活性剂,持续时间不到 2 小时,且不需要机械通气。INSURE 成功定义为 INSURE 后 72 小时内无需再次插管,INSURE 失败定义为 INSURE 后 72 小时内再次插管。不成功的 INSURE 程序定义为 INSURE 失败或表面活性剂给药后立即需要机械通气超过 24 小时。所有预测因素均在表面活性剂给药前预先定义,并存在于表面活性剂给药前。采用多变量逻辑回归。
共纳入 322 名新生儿:31%(n=100)INSURE 成功,10%(n=33)INSURE 失败,49%(n=158)需要机械通气超过 24 小时,其余 10%(n=31)需要机械通气不足 24 小时。INSURE 失败的预测因素是低胎龄和血红蛋白低于 8.5mmol/l。机械通气超过 24 小时的预测因素是低胎龄、5 分钟时 Apgar 评分低于 7、氧需求高于 50%、CO2 压高于 7kPa(~53mmHg)、pH 值低于 7.3、乳酸高于 2.5mmol/l、需要正性肌力药和表面活性剂在出生后不久给予,而子痫前期降低了风险。
我们确定了与 INSURE 程序不成功相关的特定预测因素。对于高危新生儿,有一个或多个预测因素的新生儿,在给予表面活性剂后保持插管和机械通气治疗,可能会防止再次插管。