Hites M, Taccone F S, Wolff F, Maillart E, Beumier M, Surin R, Cotton F, Jacobs F
Department of Infectious Diseases, Erasme Hospital, Université Libre de Bruxelles, Brussels, Belgium.
Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles, Brussels, Belgium.
Nutr Diabetes. 2014 Jun 23;4(6):e119. doi: 10.1038/nutd.2014.15.
Obesity may alter the pharmacokinetics of β-lactams. The goal of this study was to evaluate if and why serum concentrations are inadequate when standard β-lactam regimens are administered to obese, non-critically ill patients.
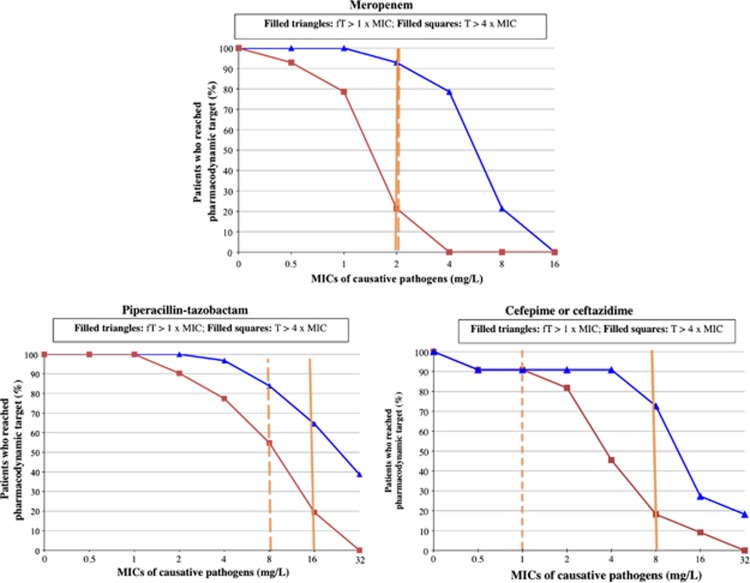
During first year, we consecutively included infected, obese patients (body mass index (BMI) ⩾30 kg m(-2)) who received meropenem (MEM), piperacillin-tazobactam (TZP) or cefepime/ceftazidime (CEF). Patients with severe sepsis or septic shock, or those hospitalized in the intensive care unit were excluded. Serum drug concentrations were measured twice during the elimination phase by high-performance liquid chromatography. We evaluated whether free or total drug concentrations were >1 time (fT>minimal inhibition concentration (MIC)) or >4 times (T>4MIC) the clinical breakpoints for Pseudomonas aeruginosa during optimal periods of time: ⩾40% for MEM, ⩾50% for TZP and ⩾70% for CEF.
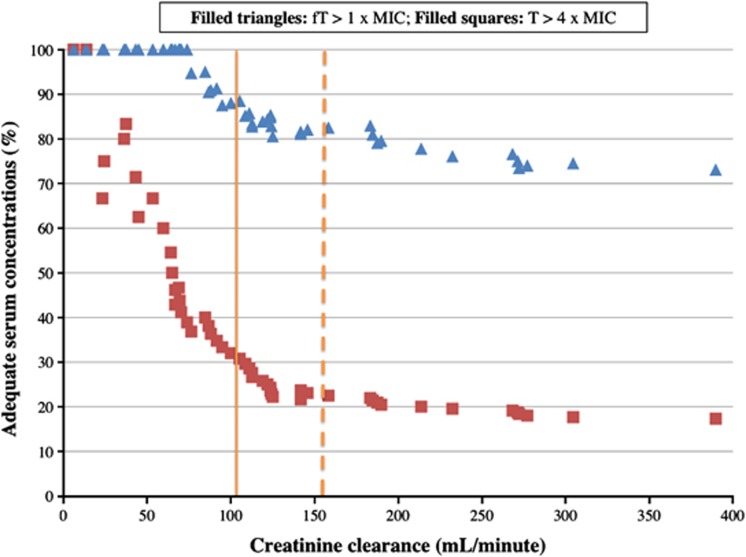
We included 56 patients (median BMI: 36 kg m(-2)): 14 received MEM, 31 TZP and 11 CEF. The percentage of patients who attained target fT>MIC and T>4MIC were 93% and 21% for MEM, 68% and 19% for TZP, and 73% and 18% for CEF, respectively. High creatinine clearance (107 (range: 6-398) ml min(-1)) was the only risk factor in univariate and multivariate analyses to predict insufficient serum concentrations.
In obese, non-critically ill patients, standard drug regimens of TZP and CEF resulted in insufficient drug concentrations to treat infections due to less susceptible bacteria. Augmented renal clearance was responsible for these low serum concentrations. New dosage regimens need to be explored in this patient population (EUDRA-CT: 2011-004239-29).
肥胖可能会改变β-内酰胺类药物的药代动力学。本研究的目的是评估在对肥胖的非危重症患者使用标准β-内酰胺类药物治疗方案时,血清浓度是否不足以及原因。
在第一年,我们连续纳入了接受美罗培南(MEM)、哌拉西林-他唑巴坦(TZP)或头孢吡肟/头孢他啶(CEF)治疗的感染肥胖患者(体重指数(BMI)⩾30 kg m(-2))。排除患有严重脓毒症或脓毒性休克的患者,或入住重症监护病房的患者。在消除阶段通过高效液相色谱法测量血清药物浓度两次。我们评估了在最佳时间段内,游离或总药物浓度是否超过铜绿假单胞菌临床断点的1倍(fT>最低抑菌浓度(MIC))或4倍(T>4MIC):MEM为⩾40%,TZP为⩾50%,CEF为⩾70%。
我们纳入了56例患者(中位BMI:36 kg m(-2)):14例接受MEM治疗,31例接受TZP治疗,11例接受CEF治疗。达到目标fT>MIC和T>4MIC的患者百分比,MEM分别为93%和21%,TZP分别为68%和19%,CEF分别为73%和18%。高肌酐清除率(107(范围:6 - 398)ml min(-1))是单因素和多因素分析中预测血清浓度不足的唯一危险因素。
在肥胖的非危重症患者中,则TZP和CEF的标准药物治疗方案导致药物浓度不足以治疗由较难感染的细菌引起的感染。肾脏清除率增加是这些低血清浓度的原因。需要在该患者群体中探索新的给药方案(欧盟临床试验注册号:2011 - 004239 - 29)。