Kitamura Hiroshi, Maeda Toshihiro, Tanaka Toshiaki, Fukuta Fumimasa, Kobayashi Ko, Nishiyama Naotaka, Takahashi Satoshi, Masumori Naoya
Department of Urology, Sapporo Medical University School of Medicine, South 1 West 16, Chuo-ku, Sapporo 060-8543, Japan.
Department of Urology, Sapporo Medical University School of Medicine, Sapporo, Japan.
JSLS. 2014 Apr-Jun;18(2):288-93. doi: 10.4293/108680813X13794522666842.
The aim of this study was to compare oncologic outcomes after laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, and open nephroureterectomy for upper urinary tract urothelial cancer.
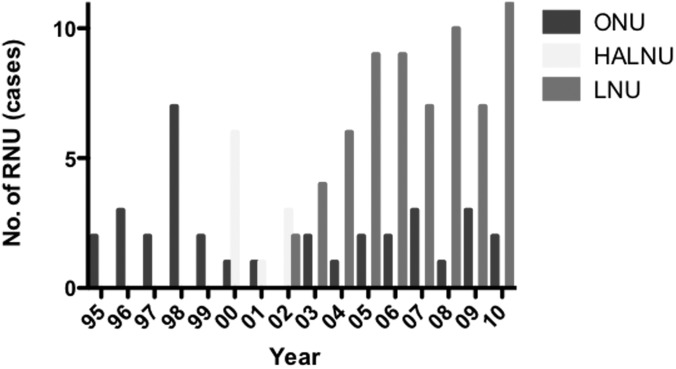
Between April 1995 and August 2010, 189 patients underwent laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, or open nephroureterectomy for upper urinary tract urothelial cancer. Of these patients, 110 with no previous or concurrent bladder cancer or any metastatic disease were included in this study. Cancer-specific survival, recurrence-free survival, and intravesical recurrence-free survival rates were analyzed by the Kaplan-Meier method and compared with the log-rank test. The median follow-up period for the cohort was 70 months (range, 6-192 months).
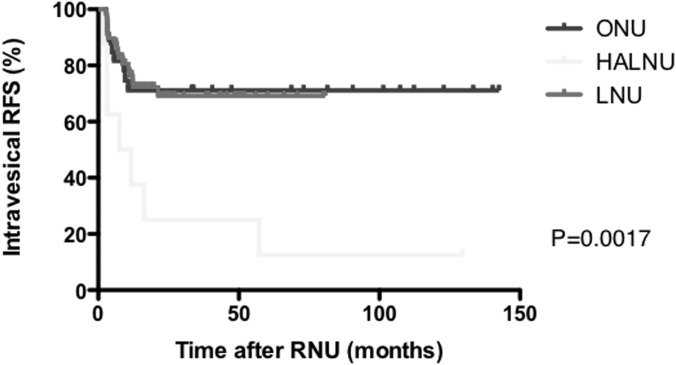
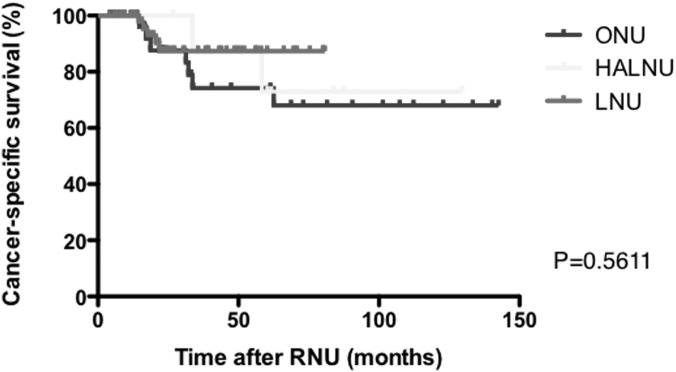
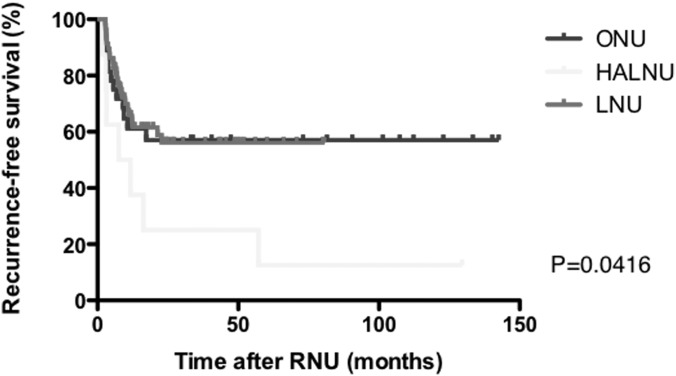
The 3 groups were well matched for tumor stage, grade, and the presence of lymphovascular invasion and concomitant carcinoma in situ. The estimated 5-year cancer-specific survival rates were 81.1%, 65.6%, and 65.2% for laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, and open nephroureterectomy, respectively (P = .4179). The estimated 5-year recurrence-free survival rates were 33.8%, 10.0%, and 41.2% for laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, and open nephroureterectomy, respectively (P = .0245). The estimated 5-year intravesical recurrence-free survival rates were 64.8%, 10.0%, and 76.2% for laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, and open nephroureterectomy, respectively (P < .0001).
Although there was no significant difference in cancer-specific survival rate among the laparoscopic nephroureterectomy, hand-assisted laparoscopic nephroureterectomy, and open nephroureterectomy groups, hand-assisted laparoscopic nephroureterectomy may be inferior to laparoscopic nephroureterectomy or open nephroureterectomy with regard to recurrence-free survival and intravesical recurrence-free survival rates.
本研究旨在比较腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术及开放性肾输尿管切除术治疗上尿路尿路上皮癌后的肿瘤学结局。
1995年4月至2010年8月期间,189例患者因上尿路尿路上皮癌接受了腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术或开放性肾输尿管切除术。其中,110例无既往或同时存在的膀胱癌或任何转移性疾病的患者被纳入本研究。采用Kaplan-Meier法分析癌症特异性生存率、无复发生存率及膀胱内无复发生存率,并通过对数秩检验进行比较。该队列的中位随访期为70个月(范围6 - 192个月)。
三组在肿瘤分期、分级、淋巴管侵犯情况及伴发原位癌方面匹配良好。腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术及开放性肾输尿管切除术的估计5年癌症特异性生存率分别为81.1%、65.6%和65.2%(P = 0.4179)。腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术及开放性肾输尿管切除术的估计5年无复发生存率分别为33.8%、10.0%和41.2%(P = 0.0245)。腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术及开放性肾输尿管切除术的估计5年膀胱内无复发生存率分别为64.8%、10.0%和76.2%(P < 0.0001)。
虽然腹腔镜肾输尿管切除术、手辅助腹腔镜肾输尿管切除术及开放性肾输尿管切除术组之间的癌症特异性生存率无显著差异,但在手辅助腹腔镜肾输尿管切除术的无复发生存率及膀胱内无复发生存率方面可能低于腹腔镜肾输尿管切除术或开放性肾输尿管切除术。