Fogang Yannick Fogoum, Camara Massaman, Diop Amadou Gallo, Ndiaye Mansour Mouhamadou
Neurology Department, Fann Teaching Hospital, Cheikh Anta Diop University, Dakar, Senegal.
BMC Neurol. 2014 Jul 1;14:138. doi: 10.1186/1471-2377-14-138.
Neurocysticercosis is a major cause of neurological symptoms in developing countries. We report a case of cerebral neurocysticercosis presenting as episodic migraine without aura, with clinico-radiological correlations and discuss the possible causal influence of neurocysticercosis on the pathomechanisms of migraine.
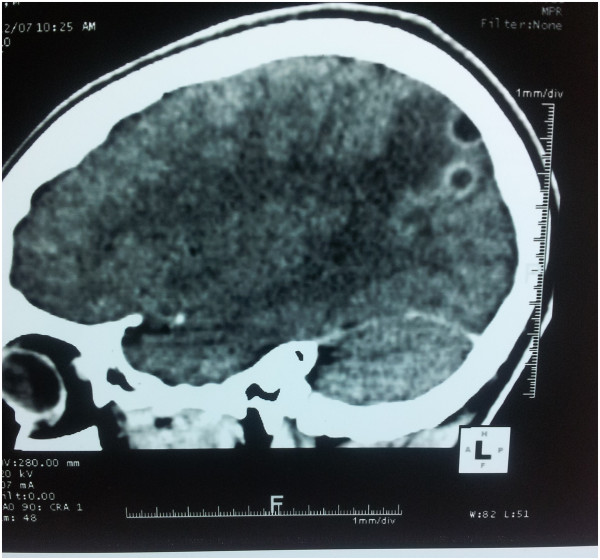
We report a 24 year-old male consulting for a one year history of recurrent headaches. He described bilateral frontal and/or temporal attacks of throbbing headache, moderate to severe in intensity, worsened by head movements and accompanied by nausea, photophobia and phonophobia. Attacks lasted between 12 and 60 hours if untreated. He never had symptoms suggestive of a migraine aura or an epileptic seizure. Headache attacks progressively increased in frequency to up to 5 to 7 severe attacks per month. On taking history, the patient reported having consumed undercooked porcine meat. Physical examination was unremarkable. A brain CT scan showed two contiguous occipital cystic lesions with ring enhancement and surrounding edema suggestive of cerebral neurocysticercosis. On laboratory work-up, blood serology for cysticercal antibodies was positive. Full blood count, erythrocyte sedimentation rate, c - reactive protein level, human immunodeficiency virus serology, liver and hepatic function were all normal. Albendazole (1000 mg/day) and prednisolone (60 mg/day) were prescribed for seven days. The patient was examined again two and six months after the end of his treatment and there was a significant reduction in headache severity and frequency.
We propose that in our patient the occipital neurocysticercosis lesions cause migraine without aura-like attacks via inflammation in the surrounding brain parenchyma leading to sensitization of the trigemino-vascular system. We cannot rule out, however, the possibility that our patient has a genetic predisposition for migraine without aura and that the fortuitous association of neurocysticercosis is simply an aggravating factor of his migraine.
神经囊尾蚴病是发展中国家神经系统症状的主要病因。我们报告一例表现为无先兆发作性偏头痛的脑型神经囊尾蚴病病例,阐述临床与影像学的相关性,并讨论神经囊尾蚴病对偏头痛发病机制可能的因果影响。
我们报告一名24岁男性,因反复发作头痛1年前来就诊。他描述双侧额部和/或颞部搏动性头痛发作,强度为中度至重度,头部活动会使其加重,并伴有恶心、畏光和畏声。若不治疗,发作持续12至60小时。他从未有过提示偏头痛先兆或癫痫发作的症状。头痛发作频率逐渐增加,每月多达5至7次严重发作。在询问病史时,患者报告曾食用未煮熟的猪肉。体格检查无异常。脑部CT扫描显示两个相邻的枕叶囊性病变,有环形强化及周围水肿,提示脑型神经囊尾蚴病。实验室检查中,囊尾蚴抗体血清学检测呈阳性。全血细胞计数、红细胞沉降率、C反应蛋白水平、人类免疫缺陷病毒血清学、肝脏及肝功能均正常。给予阿苯达唑(1000毫克/天)和泼尼松龙(60毫克/天)治疗7天。在治疗结束后2个月和6个月对患者再次进行检查,头痛的严重程度和频率显著降低。
我们认为,在我们的患者中,枕叶神经囊尾蚴病病变通过周围脑实质的炎症导致三叉神经血管系统致敏,从而引起无先兆偏头痛样发作。然而,我们不能排除患者存在无先兆偏头痛的遗传易感性,而神经囊尾蚴病的偶然关联只是其偏头痛的一个加重因素的可能性。