Lebeau Jean-Pierre, Cadwallader Jean-Sébastien, Aubin-Auger Isabelle, Mercier Alain, Pasquet Thomas, Rusch Emmanuel, Hendrickx Kristin, Vermeire Etienne
Department of General Practice, EES, University of Tours, 10 Boulevard Tonnellé, BP 3223, 37032 Tours, Cedex 1, France.
BMC Fam Pract. 2014 Jul 2;15:130. doi: 10.1186/1471-2296-15-130.
Therapeutic inertia has been defined as the failure of health-care provider to initiate or intensify therapy when therapeutic goals are not reached. It is regarded as a major cause of uncontrolled hypertension. The exploration of its causes and the interventions to reduce it are plagued by unclear conceptualizations and hypothesized mechanisms. We therefore systematically searched the literature for definitions and discussions on the concept of therapeutic inertia in hypertension in primary care, to try and form an operational definition.
A systematic review of all types of publications related to clinical inertia in hypertension was performed. Medline, EMbase, PsycInfo, the Cochrane library and databases, BDSP, CRD and NGC were searched from the start of their databases to June 2013. Articles were selected independently by two authors on the basis of their conceptual content, without other eligibility criteria or formal quality appraisal. Qualitative data were extracted independently by two teams of authors. Data were analyzed using a constant comparative qualitative method.
The final selection included 89 articles. 112 codes were grouped in 4 categories: terms and definitions (semantics), "who" (physician, patient or system), "how and why" (mechanisms and reasons), and "appropriateness". Regarding each of these categories, a number of contradictory assertions were found, most of them relying on little or no empirical data. Overall, the limits of what should be considered as inertia were not clear. A number of authors insisted that what was considered deleterious inertia might in fact be appropriate care, depending on the situation.
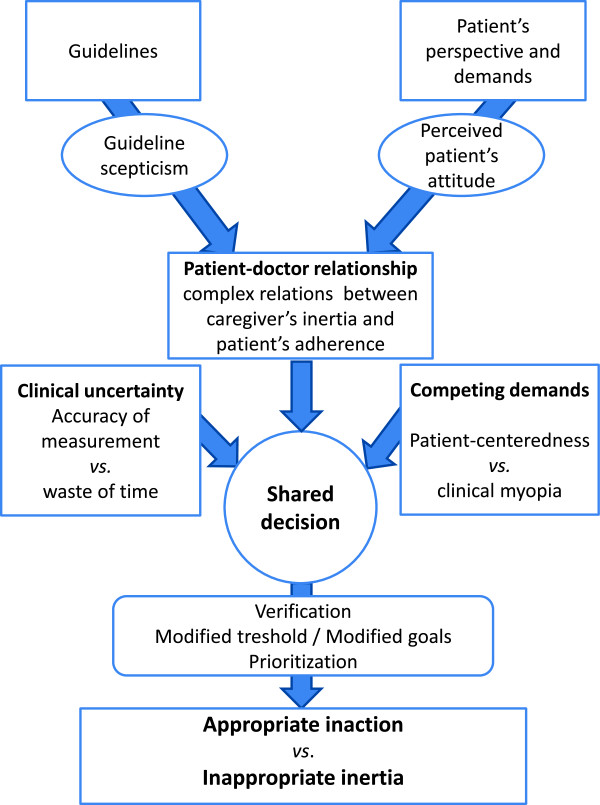
Our data analysis revealed a major lack of conceptualization of therapeutic inertia in hypertension and important discrepancies regarding its possible causes, mechanisms and outcomes. The concept should be split in two parts: appropriate inaction and inappropriate inertia. The development of consensual and operational definitions relying on empirical data and the exploration of the intimate mechanisms that underlie these behaviors are now needed.
治疗惰性被定义为当未达成治疗目标时,医疗保健提供者未能启动或强化治疗。它被视为高血压控制不佳的主要原因。对其成因及减少治疗惰性干预措施的探索,因概念不清和假设机制而受到困扰。因此,我们系统检索了文献,以查找关于基层医疗中高血压治疗惰性概念的定义和讨论,试图形成一个可操作的定义。
对所有与高血压临床惰性相关的各类出版物进行系统综述。检索了Medline、EMbase、PsycInfo、Cochrane图书馆及数据库、BDSP、CRD和NGC,时间跨度从各数据库建库起始至2013年6月。两位作者根据文章的概念内容独立筛选文章,无其他入选标准或正式的质量评估。两组作者独立提取定性数据。采用持续比较定性法对数据进行分析。
最终入选89篇文章。112个编码归为4类:术语和定义(语义)、“谁”(医生、患者或系统)、“如何及为何”(机制和原因)以及“适当性”。在每一类中,都发现了一些相互矛盾的观点,其中大多数观点几乎没有或完全没有实证数据支持。总体而言,应被视为惰性的界限并不明确。一些作者坚持认为,根据具体情况,被视为有害的惰性实际上可能是适当的治疗。
我们的数据分析显示,高血压治疗惰性在概念上存在重大缺失,在其可能的成因、机制和结果方面存在重大差异。该概念应分为两部分:适当的不作为和不适当的惰性。现在需要基于实证数据制定共识性的可操作定义,并探索这些行为背后的内在机制。