1] Department of Urology, Weill Medical College of Cornell University, New York Presbyterian Hospital, New York, NY, USA [2] Department of Urology, University Medical-Center Hamburg-Eppendorf, Hamburg, Germany.
Department of Urology, Vita-Salute San Raffaele University, Milan, Italy.
Br J Cancer. 2014 Jul 15;111(2):213-9. doi: 10.1038/bjc.2014.311. Epub 2014 Jul 8.
Pelvic lymph node dissection in patients undergoing radical prostatectomy for clinically localised prostate cancer is not without morbidity and its therapeutical benefit is still a matter of debate. The objective of this study was to develop a model that allows preoperative determination of the minimum number of lymph nodes needed to be removed at radical prostatectomy to ensure true nodal status.
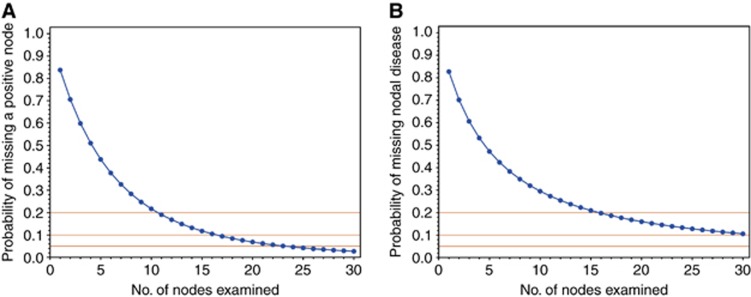
We analysed data from 4770 patients treated with radical prostatectomy and pelvic lymph node dissection between 2000 and 2011 from eight academic centres. For external validation of our model, we used data from a cohort of 3595 patients who underwent an anatomically defined extended pelvic lymph node dissection. We estimated the sensitivity of pathological nodal staging using a beta-binomial model and developed a novel clinical (preoperative) nodal staging score (cNSS), which represents the probability that a patient has lymph node metastasis as a function of the number of examined nodes.
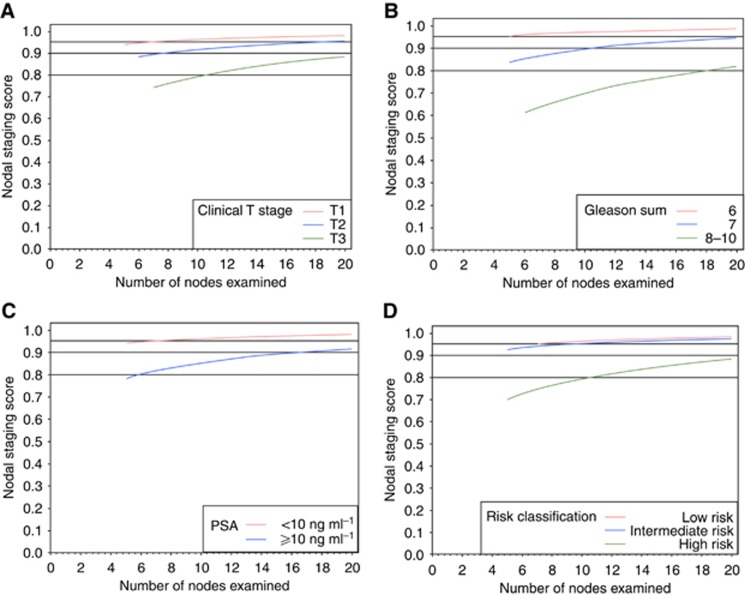
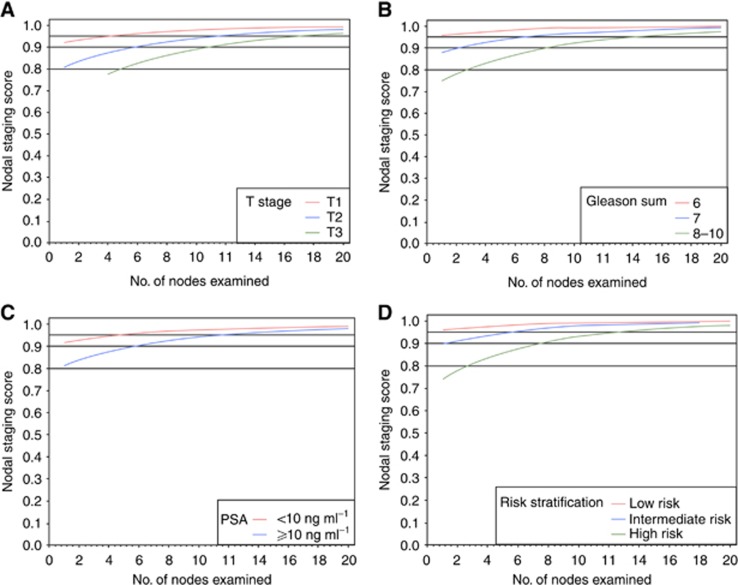
In the development and validation cohorts, the probability of missing a positive lymph node decreases with increase in the number of nodes examined. A 90% cNSS can be achieved in the development and validation cohorts by examining 1-6 nodes in cT1 and 6-8 nodes in cT2 tumours. With 11 nodes examined, patients in the development and validation cohorts achieved a cNSS of 90% and 80% with cT3 tumours, respectively.
Pelvic lymph node dissection is the only reliable technique to ensure accurate nodal staging in patients treated with radical prostatectomy for clinically localised prostate cancer. The minimum number of examined lymph nodes needed for accurate nodal staging may be predictable, being strongly dependent on prostate cancer characteristics at diagnosis.
对于接受根治性前列腺切除术治疗局部前列腺癌的患者,进行盆腔淋巴结清扫术并非没有发病率,其治疗益处仍存在争议。本研究的目的是开发一种模型,该模型可以在术前确定根治性前列腺切除术中需要切除的淋巴结的最小数量,以确保真正的淋巴结状态。
我们分析了 2000 年至 2011 年间,来自 8 个学术中心的 4770 例接受根治性前列腺切除术和盆腔淋巴结清扫术的患者的数据。为了验证我们模型的外部有效性,我们使用了 3595 例接受解剖定义的扩展盆腔淋巴结清扫术的患者队列的数据。我们使用贝塔二项式模型估计了病理淋巴结分期的敏感性,并开发了一种新的临床(术前)淋巴结分期评分(cNSS),该评分代表患者存在淋巴结转移的概率,作为检查的淋巴结数量的函数。
在开发和验证队列中,随着检查的淋巴结数量增加,漏诊阳性淋巴结的概率降低。在开发和验证队列中,通过检查 cT1 中的 1-6 个淋巴结和 cT2 中的 6-8 个淋巴结,可以实现 90%的 cNSS。通过检查 11 个淋巴结,开发和验证队列中 cT3 肿瘤患者的 cNSS 分别为 90%和 80%。
盆腔淋巴结清扫术是确保接受根治性前列腺切除术治疗局部前列腺癌的患者准确淋巴结分期的唯一可靠技术。准确的淋巴结分期所需的检查淋巴结的最小数量可能是可预测的,强烈依赖于诊断时的前列腺癌特征。