Webster Jayne, Baiden Frank, Bawah Justina, Bruce Jane, Tivura Mathilda, Delmini Rupert, Amenga-Etego Seeba, Chandramohan Daniel, Owusu-Agyei Seth
Disease Control Department, London School of Hygiene and Tropical Medicine, London, UK.
Malar J. 2014 Jul 9;13:261. doi: 10.1186/1475-2875-13-261.
The case management of febrile children in hospitals' and health centres' pre-roll out of the new WHO policy on parasitological diagnosis was assessed. The delivery of artemisinin combination therapy (ACT) at these two levels of the health system was compared.
Structured observations and exit interviews of 1,222 febrile children attending five hospitals and 861 attending ten health centres were conducted in six districts of the Brong Ahafo Region of Ghana. Effectiveness of delivery of case management of malaria was assessed. Proportions of children receiving ACT, anti-malarial monotherapy and antibiotics were described. Predictors of: a febrile child being given an ACT, a febrile child being given an antibiotic and of carers knowing how to correctly administer the ACT were assessed using logistic regression models stratified by hospitals and health centres.
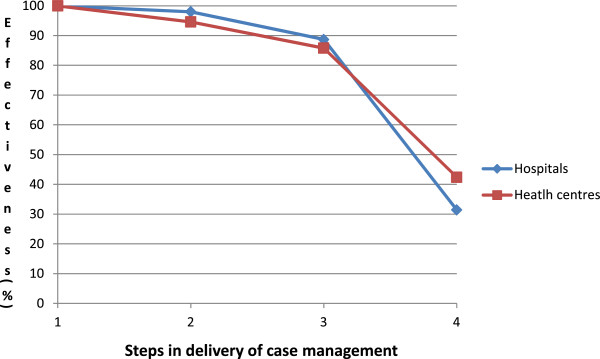
The system's effectiveness of delivering an ACT to febrile children diagnosed with malaria (parasitologically or clinically) was 31.4 and 42.4% in hospitals and health centres, respectively. The most ineffective process was that of ensuring that carers knew how to correctly administer the ACT. Overall 278 children who were not given an ACT were treated with anti-malarial monotherapy other than quinine. The majority of these children, 232/278 were given amodiaquine, 139 of these were children attending hospitals and 93 attending health centres. The cadre of health staff conducting consultation was a common predictor of the outcomes of interest. Presenting symptoms and examinations conducted were predictive of being given an ACT in hospitals and antibiotic in hospitals and health centres but not of being given an ACT in health centres. Treatment-seeking factors were predictive of being given an ACT if it was more than seven days since the fever began and an antibiotic in hospitals but not in health centres.
Interventions to improve adherence to negative parasitological tests are needed, together with guidance on dispensing of antibiotics, but improving the education of carers on how to administer ACT will lead to the greatest immediate increase in the effectiveness of case management. Guidance is needed on implementation of the new test-based treatment for malaria policy in health facilities.
对在医院和保健中心推行世界卫生组织关于寄生虫学诊断的新政策之前,发热儿童的病例管理情况进行了评估。比较了这两个卫生系统层面青蒿素联合疗法(ACT)的提供情况。
在加纳布朗阿哈福地区的六个区,对五家医院的1222名发热儿童和十家保健中心的861名发热儿童进行了结构化观察和出院访谈。评估了疟疾病例管理的提供效果。描述了接受ACT、抗疟单一疗法和抗生素治疗的儿童比例。使用按医院和保健中心分层的逻辑回归模型,评估了以下因素的预测指标:发热儿童接受ACT治疗、发热儿童接受抗生素治疗以及护理人员知道如何正确服用ACT。
在医院和保健中心,将ACT提供给经寄生虫学或临床诊断为疟疾的发热儿童的系统有效性分别为31.4%和42.4%。最无效的环节是确保护理人员知道如何正确服用ACT。总体而言,278名未接受ACT治疗的儿童接受了除奎宁以外的抗疟单一疗法。这些儿童中的大多数,即232/278,接受了阿莫地喹治疗,其中139名是在医院就诊的儿童,93名是在保健中心就诊的儿童。进行咨询的卫生工作人员类别是相关结果的常见预测指标。所呈现的症状和进行的检查可预测在医院是否接受ACT治疗以及在医院和保健中心是否接受抗生素治疗,但不能预测在保健中心是否接受ACT治疗。如果发热开始超过七天,寻求治疗的因素可预测在医院接受ACT治疗以及接受抗生素治疗,但在保健中心则不然。
需要采取干预措施提高对寄生虫学阴性检测的依从性,并提供抗生素配药指导,但提高护理人员关于如何服用ACT的教育将立即最大程度地提高病例管理的有效性。需要就卫生设施中基于新检测的疟疾治疗政策的实施提供指导。