Hogan David B, Amuah Joseph E, Strain Laurel A, Wodchis Walter P, Soo Andrea, Eliasziw Misha, Gruneir Andrea, Hagen Brad, Teare Gary, Maxwell Colleen J
David B. Hogan, MD, is a Professor and Brenda Strafford Foundation Chair in Geriatric Medicine, University of Calgary, Calgary, Alberta.
Joseph E. Amuah, PhD, is a Senior Researcher with the Health System Performance Branch, Canadian Institute for Health Information, Ottawa, Ontario.
Open Med. 2014 Mar 4;8(1):e33-45. eCollection 2014.
Little is known about health or service use outcomes for residents of Canadian assisted living facilities. Our objectives were to estimate the incidence of admission to hospital over 1 year for residents of designated (i.e., publicly funded) assisted living (DAL) facilities in Alberta, to compare this rate with the rate among residents of long-term care facilities, and to identify individual and facility predictors of hospital admission for DAL residents.
Participants were 1066 DAL residents (mean age ± standard deviation 84.9 ± 7.3 years) and 976 longterm care residents (85.4 ± 7.6 years) from the Alberta Continuing Care Epidemiological Studies (ACCES). Research nurses completed a standardized comprehensive assessment for each resident and interviewed family caregivers at baseline (2006 to 2008) and 1 year later. We used standardized interviews with administrators to generate facility- level data. We determined hospital admissions through linkage with the Alberta Inpatient Discharge Abstract Database. We used multivariable Cox proportional hazards models to identify predictors of hospital admission.
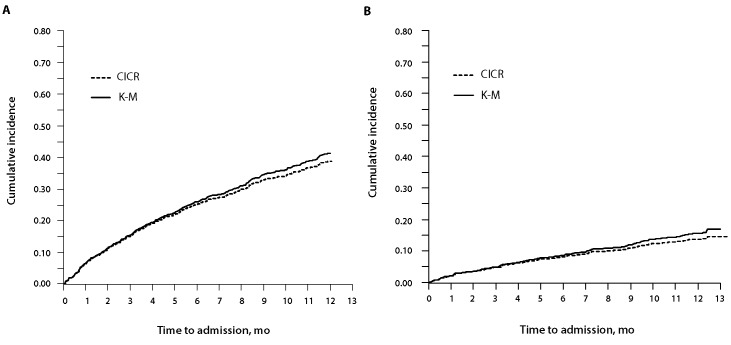
The cumulative annual incidence of hospital admission was 38.9% (95% confidence interval [CI] 35.9%- 41.9%) for DAL residents and 13.7% (95% CI 11.5%-15.8%) for long-term care residents. The risk of hospital admission was significantly greater for DAL residents with greater health instability, fatigue, medication use (11 or more medications), and 2 or more hospital admissions in the preceding year. The risk of hospital admission was also significantly higher for residents from DAL facilities with a smaller number of spaces, no licensed practical and/ or registered nurses on site (or on site less than 24 hours a day, 7 days a week), no chain affiliation, and from select health regions.
The incidence of hospital admission was about 3 times higher among DAL residents than among long-term care residents, and the risk of hospital admission was associated with a number of potentially modifiable factors. These findings raise questions about the complement of services and staffing required within assisted living facilities and the potential impact on acute care of the shift from long-term care to assisted living for the facility-based care of vulnerable older people.
对于加拿大辅助生活设施居民的健康状况或服务使用结果,我们了解得很少。我们的目标是估计艾伯塔省指定(即公共资助)辅助生活(DAL)设施居民1年内的住院发生率,将该发生率与长期护理机构居民的发生率进行比较,并确定DAL居民住院的个体和设施预测因素。
参与者来自艾伯塔省持续护理流行病学研究(ACCES),包括1066名DAL居民(平均年龄±标准差84.9±7.3岁)和976名长期护理居民(85.4±7.6岁)。研究护士为每位居民完成了标准化的综合评估,并在基线(2006年至2008年)和1年后对家庭照顾者进行了访谈。我们通过与管理人员的标准化访谈生成设施层面的数据。我们通过与艾伯塔省住院出院摘要数据库的链接确定住院情况。我们使用多变量Cox比例风险模型来确定住院的预测因素。
DAL居民的年度累计住院发生率为38.9%(95%置信区间[CI]35.9%-41.9%),长期护理居民为13.7%(95%CI 11.5%-15.8%)。健康状况不稳定、疲劳、使用药物(11种或更多药物)以及前一年有2次或更多次住院经历的DAL居民住院风险显著更高。空间较少、现场没有执业护士和/或注册护士(或每周7天每天现场工作时间少于24小时)、没有连锁附属关系以及来自特定健康区域的DAL设施居民住院风险也显著更高。
DAL居民的住院发生率约为长期护理居民的3倍,住院风险与一些可能可改变的因素有关。这些发现引发了关于辅助生活设施所需服务和人员配置的补充以及从长期护理转向辅助生活对弱势老年人机构护理急性护理的潜在影响的问题。