Ryan Jennifer M, Walsh Michael, Gormley John
School of Medicine, Trinity College Dublin, Dublin, Ireland.
J Neuroeng Rehabil. 2014 Aug 5;11:116. doi: 10.1186/1743-0003-11-116.
Advanced accelerometry-based devices have the potential to improve the measurement of everyday energy expenditure (EE) in people with cerebral palsy (CP). The aim of this study was to investigate the ability of two such devices (the Sensewear ProArmband and the Intelligent Device for Energy Expenditure and Activity) and the ability of a traditional accelerometer (the RT3) to estimate EE in adults and children with CP.
Adults (n = 18; age 31.9 ± 9.5 yr) and children (n = 18; age 11.4 ± 3.2 yr) with CP (GMFCS levels I-III) participated in this study. Oxygen uptake, measured by the Oxycon Mobile portable indirect calorimeter, was converted into EE using Weir's equation and used as the criterion measure. Participants' EE was measured simultaneously with the indirect calorimeter and three accelerometers while they rested for 10 minutes in a supine position, walked overground at a maximal effort for 6 minutes, and completed four treadmill activities for 5 minutes each at speeds of 1.0 km.h⁻¹, 1.0 km.h⁻¹ at 5% incline, 2.0 km.h⁻¹, and 4.0 km.h⁻¹.
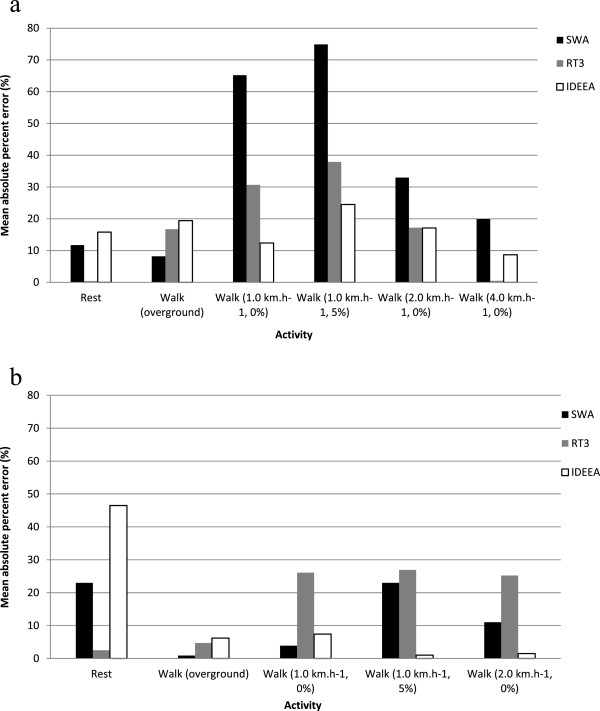
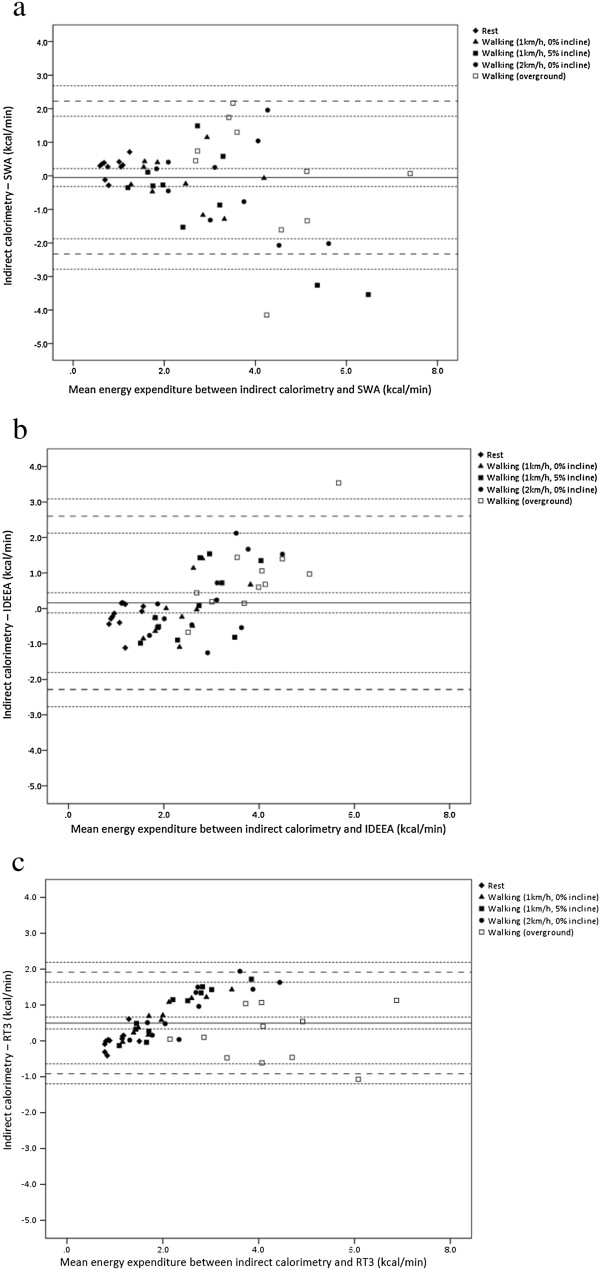
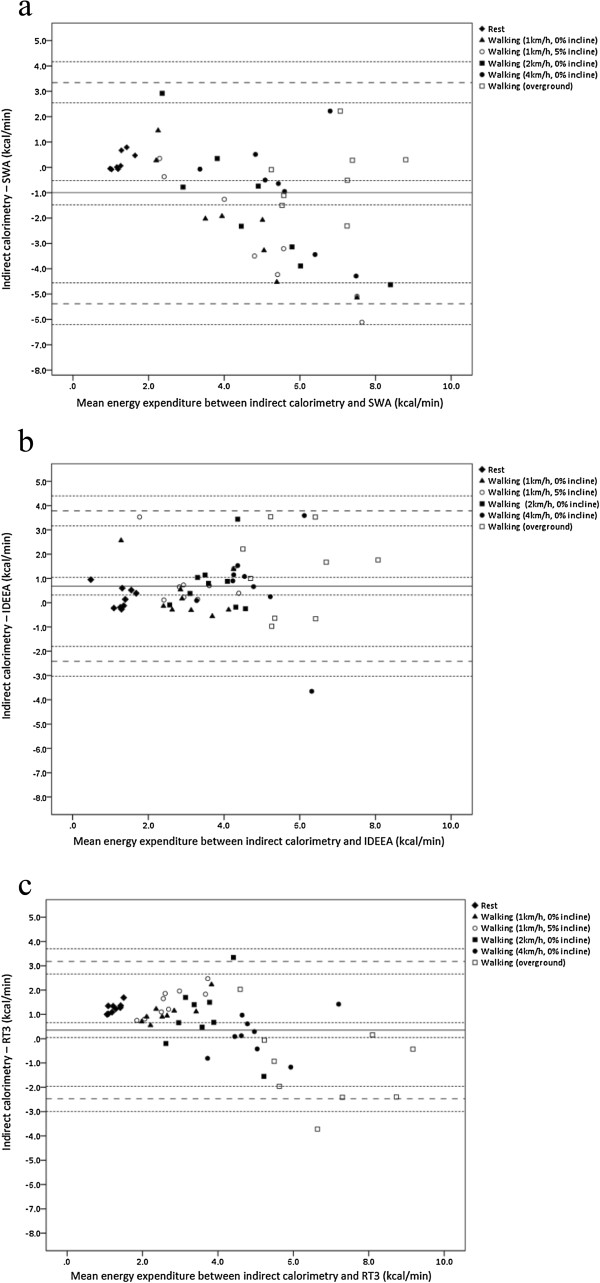
In adults the mean absolute percentage error was smallest for the IDEEA, ranging from 8.4% to 24.5% for individual activities (mean 16.3%). In children the mean absolute percentage error was smallest for the SWA, ranging from 0.9% to 23.0% for individual activities (mean 12.4%). Limits of agreement revealed that the RT3 provided the best agreement with the indirect calorimeter for adults and children. The upper and lower limits of agreement for adults were 3.18 kcal.min⁻¹ (95% CI = 2.66 to 3.70 kcal.min⁻¹) and -2.47 kcal.min⁻¹ (95% CI = -1.95 to -3.00 kcal.min⁻¹), respectively. For children, the upper and lower limits of agreement were 1.91 kcal.min⁻¹ (1.64 to 2.19 kcal.min⁻¹) and -0.92 kcal.min⁻¹ (95% CI = -1.20 to -0.64 kcal.min⁻¹) respectively. These limits of agreement represent -67.2% to 86.3% of mean EE for adults and -36.5% to 76.3% of mean EE for children, respectively.
Although the RT3 provided the best agreement with the indirect calorimeter the RT3 could significantly overestimate or underestimate individual estimates of EE. The development of CP-specific algorithms may improve the ability of these devices to estimate EE in this population.
基于先进加速度测量技术的设备有潜力改善对脑瘫(CP)患者日常能量消耗(EE)的测量。本研究的目的是调查两种此类设备(Sensewear Pro臂带和能量消耗与活动智能设备)以及传统加速度计(RT3)估计CP成人和儿童EE的能力。
患有CP(GMFCS分级I - III级)的成人(n = 18;年龄31.9±9.5岁)和儿童(n = 18;年龄11.4±3.2岁)参与了本研究。通过Oxycon Mobile便携式间接测热仪测量的摄氧量,使用韦尔方程转换为EE,并用作标准测量值。在参与者仰卧休息10分钟、以最大努力在平地上行走6分钟以及在跑步机上以1.0 km.h⁻¹、1.0 km.h⁻¹且坡度为5%、2.0 km.h⁻¹和4.0 km.h⁻¹的速度分别完成四项5分钟的活动时,同时使用间接测热仪和三种加速度计测量他们的EE。
在成人中,IDEEA的平均绝对百分比误差最小,个体活动的误差范围为8.4%至24.5%(平均16.3%)。在儿童中,SWA的平均绝对百分比误差最小,个体活动的误差范围为0.9%至23.0%(平均12.4%)。一致性界限表明,RT3与成人和儿童的间接测热仪一致性最佳。成人的一致性上限和下限分别为3.18 kcal.min⁻¹(95% CI = 2.66至3.70 kcal.min⁻¹)和 -2.47 kcal.min⁻¹(95% CI = -1.95至 -3.00 kcal.min⁻¹)。对于儿童,一致性上限和下限分别为1.91 kcal.min⁻¹(1.64至2.19 kcal.min⁻¹)和 -0.92 kcal.min⁻¹(95% CI = -1.20至 -0.64 kcal.min⁻¹)。这些一致性界限分别占成人平均EE的 -67.2%至86.3%和儿童平均EE的 -36.5%至76.3%。
尽管RT3与间接测热仪的一致性最佳,但RT3可能会显著高估或低估EE的个体估计值。开发针对CP的特定算法可能会提高这些设备在该人群中估计EE的能力。