Espeland Mark A, Glick Henry A, Bertoni Alain, Brancati Frederick L, Bray George A, Clark Jeanne M, Curtis Jeffrey M, Egan Caitlin, Evans Mary, Foreyt John P, Ghazarian Siran, Gregg Edward W, Hazuda Helen P, Hill James O, Hire Don, Horton Edward S, Hubbard Van S, Jakicic John M, Jeffery Robert W, Johnson Karen C, Kahn Steven E, Killean Tina, Kitabchi Abbas E, Knowler William C, Kriska Andrea, Lewis Cora E, Miller Marsha, Montez Maria G, Murillo Anne, Nathan David M, Nyenwe Ebenezer, Patricio Jennifer, Peters Anne L, Pi-Sunyer Xavier, Pownall Henry, Redmon J Bruce, Rushing Julia, Ryan Donna H, Safford Monika, Tsai Adam G, Wadden Thomas A, Wing Rena R, Yanovski Susan Z, Zhang Ping
Department of Biostatistical Sciences, Wake Forest School of Medicine, Winston-Salem, NC
Weight and Eating Disorder Program, University of Pennsylvania, Philadelphia, PA.
Diabetes Care. 2014 Sep;37(9):2548-56. doi: 10.2337/dc14-0093.
To assess the relative impact of an intensive lifestyle intervention (ILI) on use and costs of health care within the Look AHEAD trial.
A total of 5,121 overweight or obese adults with type 2 diabetes were randomly assigned to an ILI that promoted weight loss or to a comparison condition of diabetes support and education (DSE). Use and costs of health-care services were recorded across an average of 10 years.
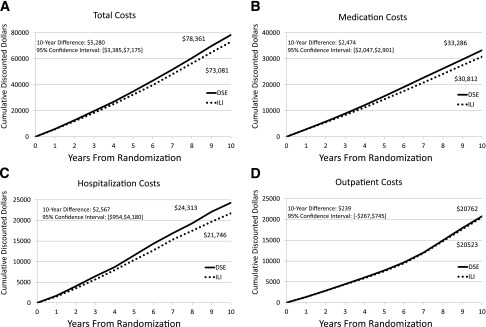
ILI led to reductions in annual hospitalizations (11%, P = 0.004), hospital days (15%, P = 0.01), and number of medications (6%, P < 0.001), resulting in cost savings for hospitalization (10%, P = 0.04) and medication (7%, P < 0.001). ILI produced a mean relative per-person 10-year cost savings of $5,280 (95% CI 3,385-7,175); however, these were not evident among individuals with a history of cardiovascular disease.
Compared with DSE over 10 years, ILI participants had fewer hospitalizations, fewer medications, and lower health-care costs.
在“展望未来”(Look AHEAD)试验中评估强化生活方式干预(ILI)对医疗保健使用情况和成本的相对影响。
共有5121名超重或肥胖的2型糖尿病成年人被随机分配至促进体重减轻的ILI组或糖尿病支持与教育(DSE)对照组。平均在10年期间记录医疗保健服务的使用情况和成本。
ILI导致年度住院次数减少(11%,P = 0.004)、住院天数减少(15%,P = 0.01)以及药物数量减少(6%,P < 0.001),从而使住院成本节省10%(P = 0.04),药物成本节省7%(P < 0.001)。ILI使人均10年成本平均相对节省5280美元(95%置信区间3385 - 7175美元);然而,在有心血管疾病史的个体中这些节省并不明显。
与10年的DSE相比,ILI参与者的住院次数更少、用药更少且医疗保健成本更低。