Liu Nan, Koh Zhi Xiong, Goh Junyang, Lin Zhiping, Haaland Benjamin, Ting Boon Ping, Ong Marcus Eng Hock
Department of Emergency Medicine, Singapore General Hospital, Outram Road, Singapore 169608, Singapore.
BMC Med Inform Decis Mak. 2014 Aug 23;14:75. doi: 10.1186/1472-6947-14-75.
The key aim of triage in chest pain patients is to identify those with high risk of adverse cardiac events as they require intensive monitoring and early intervention. In this study, we aim to discover the most relevant variables for risk prediction of major adverse cardiac events (MACE) using clinical signs and heart rate variability.
A total of 702 chest pain patients at the Emergency Department (ED) of a tertiary hospital in Singapore were included in this study. The recruited patients were at least 30 years of age and who presented to the ED with a primary complaint of non-traumatic chest pain. The primary outcome was a composite of MACE such as death and cardiac arrest within 72 h of arrival at the ED. For each patient, eight clinical signs such as blood pressure and temperature were measured, and a 5-min ECG was recorded to derive heart rate variability parameters. A random forest-based novel method was developed to select the most relevant variables. A geometric distance-based machine learning scoring system was then implemented to derive a risk score from 0 to 100.
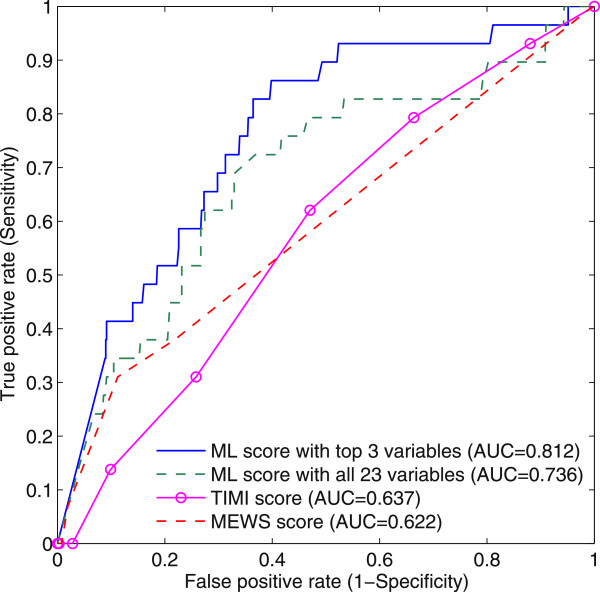
Out of 702 patients, 29 (4.1%) met the primary outcome. We selected the 3 most relevant variables for predicting MACE, which were systolic blood pressure, the mean RR interval and the mean instantaneous heart rate. The scoring system with these 3 variables produced an area under the curve (AUC) of 0.812, and a cutoff score of 43 gave a sensitivity of 82.8% and specificity of 63.4%, while the scoring system with all the 23 variables had an AUC of 0.736, and a cutoff score of 49 gave a sensitivity of 72.4% and specificity of 63.0%. Conventional thrombolysis in myocardial infarction score and the modified early warning score achieved AUC values of 0.637 and 0.622, respectively.
It is observed that a few predictors outperformed the whole set of variables in predicting MACE within 72 h. We conclude that more predictors do not necessarily guarantee better prediction results. Furthermore, machine learning-based variable selection seems promising in discovering a few relevant and significant measures as predictors.
胸痛患者分诊的关键目标是识别那些有发生不良心脏事件高风险的患者,因为他们需要强化监测和早期干预。在本研究中,我们旨在利用临床体征和心率变异性来发现预测主要不良心脏事件(MACE)最相关的变量。
新加坡一家三级医院急诊科的702例胸痛患者纳入本研究。纳入的患者年龄至少30岁,因非创伤性胸痛为主诉就诊于急诊科。主要结局是到达急诊科72小时内的MACE复合结局,如死亡和心脏骤停。对每位患者测量8项临床体征,如血压和体温,并记录5分钟心电图以得出心率变异性参数。开发了一种基于随机森林的新方法来选择最相关的变量。然后实施基于几何距离的机器学习评分系统以得出0至100的风险评分。
702例患者中,29例(4.1%)符合主要结局。我们选择了预测MACE最相关的3个变量,即收缩压、平均RR间期和平均瞬时心率。包含这3个变量的评分系统曲线下面积(AUC)为0.812,截断分数为43时,敏感性为82.8%,特异性为63.4%,而包含所有23个变量的评分系统AUC为0.736,截断分数为49时,敏感性为72.4%,特异性为63.0%。传统的心肌梗死溶栓评分和改良早期预警评分的AUC值分别为0.637和0.622。
观察到在预测72小时内的MACE时,少数预测指标比整个变量集表现更好。我们得出结论,更多的预测指标不一定能保证更好的预测结果。此外,基于机器学习的变量选择在发现一些相关且重要的指标作为预测指标方面似乎很有前景。