Ramli Anis S, Lakshmanan Sharmila, Haniff Jamaiyah, Selvarajah Sharmini, Tong Seng F, Bujang Mohamad-Adam, Abdul-Razak Suraya, Shafie Asrul A, Lee Verna K M, Abdul-Rahman Thuhairah H, Daud Maryam H, Ng Kien K, Ariffin Farnaza, Abdul-Hamid Hasidah, Mazapuspavina Md-Yasin, Mat-Nasir Nafiza, Miskan Maizatullifah, Stanley-Ponniah Jaya P, Ismail Mastura, Chan Chun W, Abdul-Rahman Yong R, Chew Boon-How, Low Wilson H H
Primary Care Medicine Discipline, Faculty of Medicine, Universiti Teknologi MARA, Selayang Campus, 68100 Batu Caves, Selangor, Malaysia.
BMC Fam Pract. 2014 Sep 13;15:151. doi: 10.1186/1471-2296-15-151.
Chronic disease management presents enormous challenges to the primary care workforce because of the rising epidemic of cardiovascular risk factors. The chronic care model was proven effective in improving chronic disease outcomes in developed countries, but there is little evidence of its effectiveness in developing countries. The aim of this study was to evaluate the effectiveness of the EMPOWER-PAR intervention (multifaceted chronic disease management strategies based on the chronic care model) in improving outcomes for type 2 diabetes mellitus and hypertension using readily available resources in the Malaysian public primary care setting. This paper presents the study protocol.
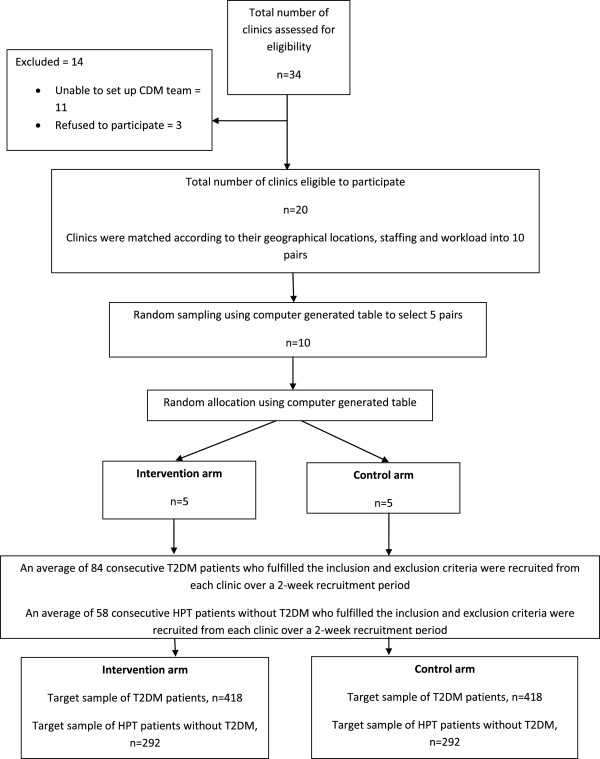
METHODS/DESIGN: A pragmatic cluster randomised controlled trial using participatory action research is underway in 10 public primary care clinics in Selangor and Kuala Lumpur, Malaysia. Five clinics were randomly selected to provide the EMPOWER-PAR intervention for 1 year and another five clinics continued with usual care. Each clinic consecutively recruits type 2 diabetes mellitus and hypertension patients fulfilling the inclusion and exclusion criteria over a 2-week period. The EMPOWER-PAR intervention consists of creating/strengthening a multidisciplinary chronic disease management team, training the team to use the Global Cardiovascular Risks Self-Management Booklet to support patient care and reinforcing the use of relevant clinical practice guidelines for management and prescribing. For type 2 diabetes mellitus, the primary outcome is the change in the proportion of patients achieving HbA1c < 6.5%. For hypertension without type 2 diabetes mellitus, the primary outcome is the change in the proportion of patients achieving blood pressure < 140/90 mmHg. Secondary outcomes include the proportion of patients achieving targets for serum lipid profile, body mass index and waist circumference. Other outcome measures include medication adherence levels, process of care and prescribing patterns. Patients' assessment of their chronic disease care and providers' perceptions, attitudes and perceived barriers in care delivery and cost-effectiveness of the intervention are also evaluated.
Results from this study will provide objective evidence of the effectiveness and cost-effectiveness of a multifaceted intervention based on the chronic care model in resource-constrained public primary care settings. The evidence should instigate crucial primary care system change in Malaysia.
ClinicalTrials.gov NCT01545401.
由于心血管危险因素的流行趋势不断上升,慢性病管理给基层医疗工作者带来了巨大挑战。慢性病护理模式在发达国家被证明能有效改善慢性病治疗效果,但在发展中国家,其有效性的证据却很少。本研究的目的是评估“赋能-患者积极参与”干预措施(基于慢性病护理模式的多方面慢性病管理策略)在马来西亚公共基层医疗环境中利用现有资源改善2型糖尿病和高血压治疗效果的有效性。本文介绍了该研究方案。
方法/设计:一项采用参与式行动研究的实用整群随机对照试验正在马来西亚雪兰莪州和吉隆坡的10家公共基层医疗诊所进行。随机选择5家诊所提供为期1年的“赋能-患者积极参与”干预措施,另外5家诊所继续提供常规护理。每家诊所连续两周招募符合纳入和排除标准的2型糖尿病和高血压患者。“赋能-患者积极参与”干预措施包括组建/加强多学科慢性病管理团队、培训团队使用《全球心血管风险自我管理手册》以支持患者护理,以及加强使用相关临床实践指南进行管理和开药。对于2型糖尿病,主要结局是糖化血红蛋白(HbA1c)<6.5%的患者比例变化。对于无2型糖尿病的高血压患者,主要结局是血压<140/90 mmHg的患者比例变化。次要结局包括达到血脂谱、体重指数和腰围目标的患者比例。其他结局指标包括药物依从性水平、护理过程和开药模式。还评估了患者对其慢性病护理的评估以及提供者对护理提供的看法、态度和感知障碍,以及干预措施的成本效益。
本研究结果将为基于慢性病护理模式的多方面干预措施在资源有限的公共基层医疗环境中的有效性和成本效益提供客观证据。这些证据应促使马来西亚基层医疗系统发生关键变革。
ClinicalTrials.gov NCT01545401