Nilsson Lennart, Wieringa Wouter G, Pundziute Gabija, Gjerde Marcus, Engvall Jan, Swahn Eva, Jonasson Lena
Department of Medical and Health Sciences, Linköping University, Linköping, Sweden; Department of Cardiology, Linköping University, Linköping, Sweden.
University of Groningen, University Medical Center Groningen, Department of Cardiology, Groningen, The Netherlands.
PLoS One. 2014 Sep 30;9(9):e108183. doi: 10.1371/journal.pone.0108183. eCollection 2014.
Elevations in soluble markers of inflammation and changes in leukocyte subset distribution are frequently reported in patients with coronary artery disease (CAD). Lately, the neutrophil/lymphocyte ratio has emerged as a potential marker of both CAD severity and cardiovascular prognosis.
The aim of the study was to investigate whether neutrophil/lymphocyte ratio and other immune-inflammatory markers were related to plaque burden, as assessed by coronary computed tomography angiography (CCTA), in patients with CAD.
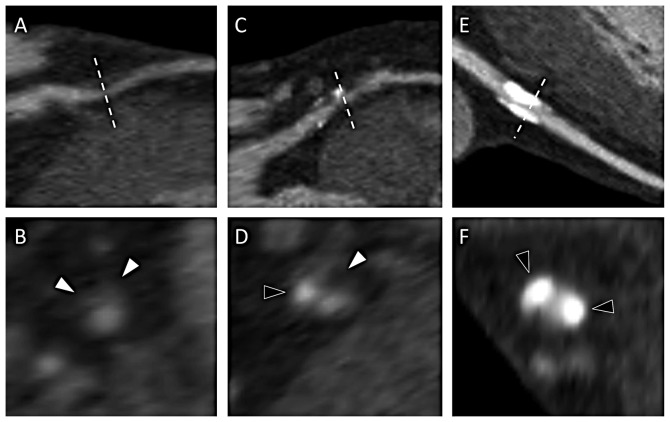
Twenty patients with non-ST-elevation acute coronary syndrome (NSTE-ACS) and 30 patients with stable angina (SA) underwent CCTA at two occasions, immediately prior to coronary angiography and after three months. Atherosclerotic plaques were classified as calcified, mixed and non-calcified. Blood samples were drawn at both occasions. Leukocyte subsets were analyzed by white blood cell differential counts and flow cytometry. Levels of C-reactive protein (CRP) and interleukin(IL)-6 were measured in plasma. Blood analyses were also performed in 37 healthy controls.
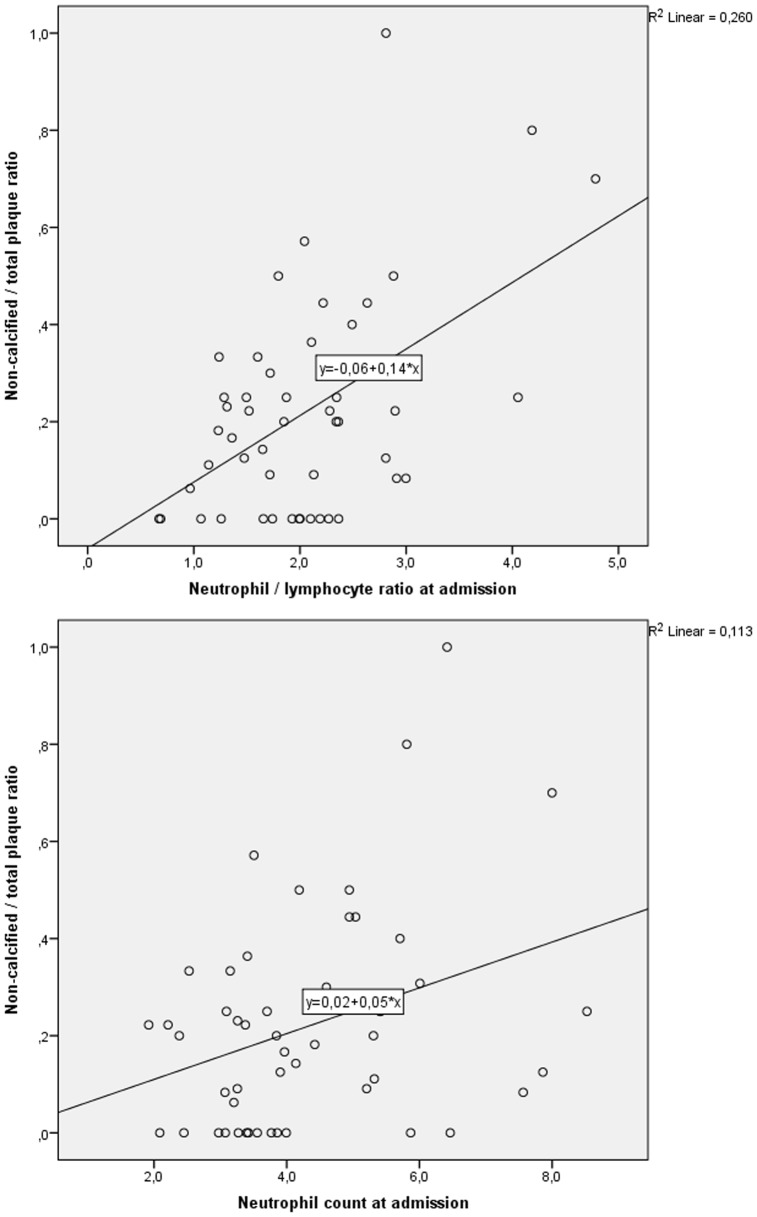
Plaque variables did not change over 3 months, total plaque burden being similar in NSTE-ACS and SA. However, non-calcified/total plaque ratio was higher in NSTE-ACS, 0.25(0.09-0.44) vs 0.11(0.00-0.25), p<0.05. At admission, levels of monocytes, neutrophils, neutrophil/lymphocyte ratios, CD4+ T cells, CRP and IL-6 were significantly elevated, while levels of NK cells were reduced, in both patient groups as compared to controls. After 3 months, levels of monocytes, neutrophils, neutrophil/lymphocyte ratios and CD4+ T cells remained elevated in patients. Neutrophil/lymphocyte ratios and neutrophil counts correlated significantly with numbers of non-calcified plaques and also with non-calcified/total plaque ratio (r = 0.403, p = 0.010 and r = 0.382, p = 0.024, respectively), but not with total plaque burden.
Among immune-inflammatory markers in NSTE-ACS and SA patients, neutrophil counts and neutrophil/lymphocyte ratios were significantly correlated with non-calcified plaques. Data suggest that these easily measured biomarkers reflect the burden of vulnerable plaques in CAD.
炎症可溶性标志物升高以及白细胞亚群分布变化在冠心病(CAD)患者中经常被报道。最近,中性粒细胞/淋巴细胞比值已成为CAD严重程度和心血管预后的潜在标志物。
本研究旨在调查在CAD患者中,中性粒细胞/淋巴细胞比值和其他免疫炎症标志物是否与通过冠状动脉计算机断层扫描血管造影(CCTA)评估的斑块负荷相关。
20例非ST段抬高型急性冠状动脉综合征(NSTE-ACS)患者和30例稳定型心绞痛(SA)患者在两个时间点接受了CCTA检查,分别在冠状动脉造影前即刻和三个月后。动脉粥样硬化斑块被分类为钙化斑块、混合斑块和非钙化斑块。在两个时间点均采集血样。通过白细胞分类计数和流式细胞术分析白细胞亚群。检测血浆中C反应蛋白(CRP)和白细胞介素(IL)-6的水平。还对37名健康对照者进行了血液分析。
斑块变量在3个月内没有变化,NSTE-ACS和SA患者的总斑块负荷相似。然而,NSTE-ACS患者的非钙化/总斑块比值更高,分别为0.25(0.09 - 0.44)和0.11(0.00 - 0.25),p<0.05。入院时,与对照组相比,两个患者组的单核细胞、中性粒细胞、中性粒细胞/淋巴细胞比值、CD4 + T细胞、CRP和IL-6水平均显著升高,而NK细胞水平降低。3个月后,患者的单核细胞、中性粒细胞、中性粒细胞/淋巴细胞比值和CD4 + T细胞水平仍保持升高。中性粒细胞/淋巴细胞比值和中性粒细胞计数与非钙化斑块数量以及非钙化/总斑块比值显著相关(r分别为0.403,p = 0.010和r = 0.382,p = 0.024),但与总斑块负荷无关。
在NSTE-ACS和SA患者的免疫炎症标志物中,中性粒细胞计数和中性粒细胞/淋巴细胞比值与非钙化斑块显著相关。数据表明,这些易于测量的生物标志物反映了CAD中易损斑块的负荷。