Department of Physical Medicine and Rehabilitation, Program in Physical Therapy, University of Minnesota, Medical School Minneapolis, MN, USA.
Alberta Children's Hospital Research Institute, University of Calgary Calgary, AB, Canada.
Front Hum Neurosci. 2014 Sep 19;8:739. doi: 10.3389/fnhum.2014.00739. eCollection 2014.
Transcranial direct current stimulation (tDCS) has been investigated mainly in adults and doses may not be appropriate in pediatric applications. In perinatal stroke where potential applications are promising, rational adaptation of dosage for children remains under investigation.
Construct child-specific tDCS dosing parameters through case study within a perinatal stroke tDCS safety and feasibility trial.
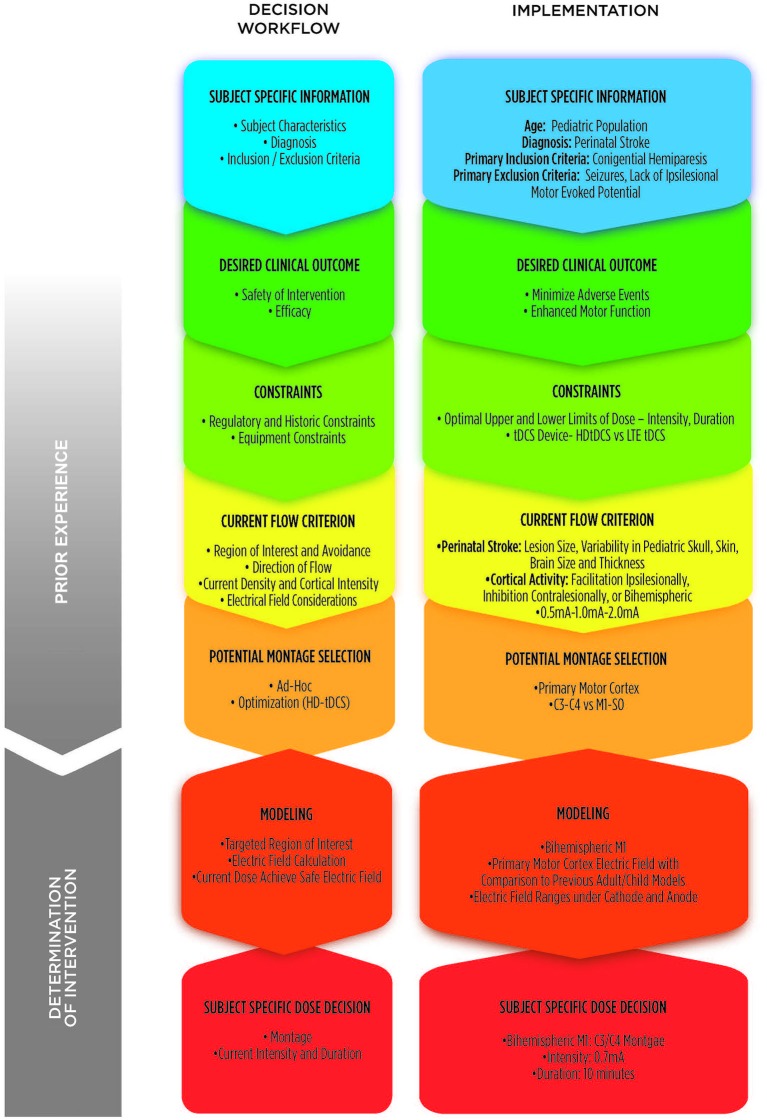
10-year-old subject with a diagnosis of presumed perinatal ischemic stroke and hemiparesis was identified. T1 magnetic resonance imaging (MRI) scans used to derive computerized model for current flow and electrode positions. Workflow using modeling results and consideration of dosage in previous clinical trials was incorporated. Prior ad hoc adult montages vs. de novo optimized montages provided distinct risk benefit analysis. Approximating adult dose required consideration of changes in both peak brain current flow and distribution which further tradeoff between maximizing efficacy and adding safety factors. Electrode size, position, current intensity, compliance voltage, and duration were controlled independently in this process.
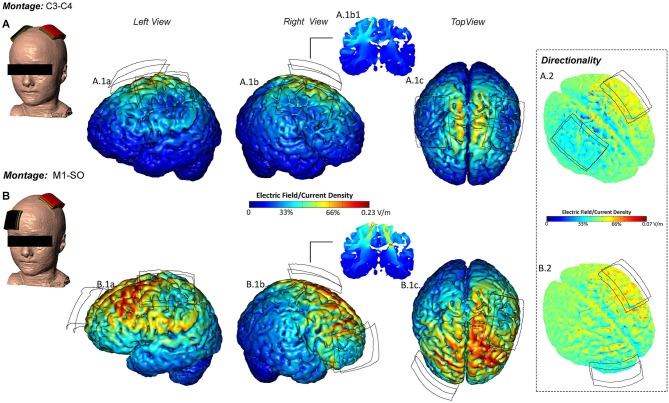
Brain electric fields modeled and compared to values previously predicted models (Datta et al., 2011; Minhas et al., 2012). Approximating conservative brain current flow patterns and intensities used in previous adult trials for comparable indications, the optimal current intensity established was 0.7 mA for 10 min with a tDCS C3/C4 montage. Specifically 0.7 mA produced comparable peak brain current intensity of an average adult receiving 1.0 mA. Electrode size of 5 × 7 cm(2) with 1.0 mA and low-voltage tDCS was employed to maximize tolerability. Safety and feasibility confirmed with subject tolerating the session well and no serious adverse events.
Rational approaches to dose customization, with steps informed by computational modeling, may improve guidance for pediatric stroke tDCS trials.
经颅直流电刺激(tDCS)主要在成年人中进行了研究,其剂量在儿科应用中可能并不合适。在潜在应用前景广阔的围产期卒中中,儿童剂量的合理适应仍在研究中。
通过围产期卒中 tDCS 安全性和可行性试验中的案例研究,构建儿童特异性 tDCS 剂量参数。
确定了一名患有疑似围产期缺血性卒中伴偏瘫的 10 岁儿童患者。使用 T1 磁共振成像(MRI)扫描来推导电流流动和电极位置的计算机模型。该方法结合了建模结果和之前临床试验中的剂量考虑因素,使用了先前的特定成人组合与新优化的组合,提供了不同的风险效益分析。近似成人剂量需要考虑峰值脑电流流动和分布的变化,这进一步在最大化疗效和增加安全因素之间进行权衡。在这个过程中,独立控制了电极尺寸、位置、电流强度、顺应电压和持续时间。
对建模后的脑电场与之前预测模型(Datta 等人,2011 年;Minhas 等人,2012 年)进行了比较。近似于之前成人试验中用于类似适应证的保守脑电流流动模式和强度,确定的最佳电流强度为 0.7 mA,持续 10 分钟,采用 C3/C4 电极组合。具体来说,0.7 mA 产生的平均成人接受 1.0 mA 的峰值脑电流强度相当。采用 5×7 cm2 的电极尺寸和 1.0 mA 及低电压 tDCS,以提高耐受性。该方法安全且可行,受试儿童耐受良好,未发生严重不良事件。
通过计算建模提供信息的剂量定制合理方法,可能会为儿科卒中 tDCS 试验提供更好的指导。