Bisschops Laurens L A, van der Hoeven Johannes G, Mollnes Tom E, Hoedemaekers Cornelia W E
Department of Intensive Care, Radboud University Nijmegen Medical Centre, PO Box 9101, Nijmegen, 6500 HB, The Netherlands.
Institute of Immunology, Oslo University Hospital and University of Oslo, P.B. 4950, Nydalen, N-0424, Oslo, Norway.
Crit Care. 2014 Oct 11;18(5):546. doi: 10.1186/s13054-014-0546-5.
Whole-body ischemia and reperfusion trigger a systemic inflammatory response. In this study, we analyzed the effect of temperature on the inflammatory response in patients treated with prolonged mild hypothermia after cardiac arrest.
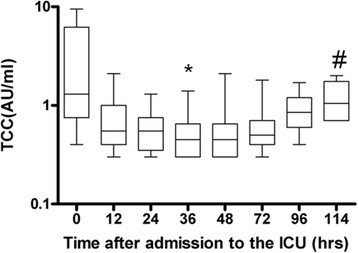
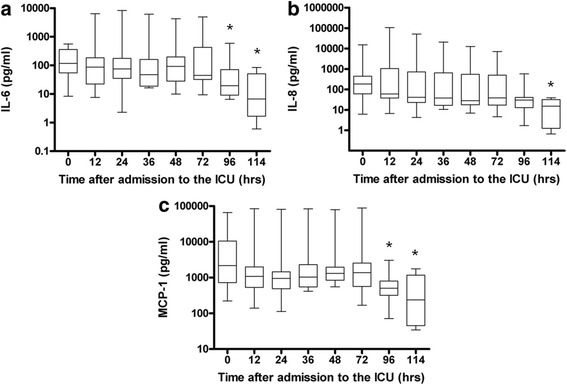
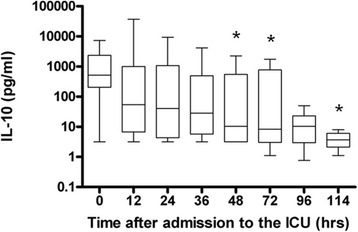
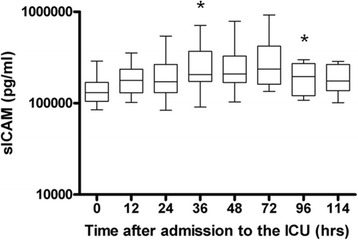
Ten comatose patients with return of spontaneous circulation after pulseless electrical activity/asystole or prolonged ventricular fibrillation were treated with mild therapeutic hypothermia for 72 hours after admission to a tertiary care university hospital. At admission and at 12, 24, 36, 48, 72, 96 and 114 hours, the patients' temperature was measured and blood samples were taken from the arterial catheter. Proinflammatory interleukin 6 (IL-6) and anti-inflammatory (IL-10) cytokines and chemokines (IL-8 and monocyte chemotactic protein 1), intercellular adhesion molecule 1 and complement activation products (C1r-C1s-C1inhibitor, C4bc, C3bPBb, C3bc and terminal complement complex) were measured. Changes over time were analyzed with the repeated measures test for nonparametric data. Dunn's multiple comparisons test was used for comparison of individual time points.
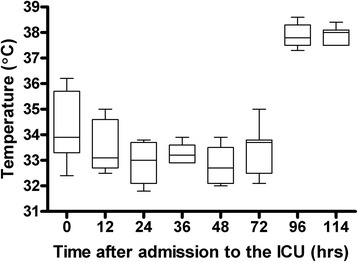
The median temperature at the start of the study was 34.3°C (33.4°C to 35.2°C) and was maintained between 32°C and 34°C for 72 hours. All patients were passively rewarmed after 72 hours, from (median (IQR)) 33.7°C (33.1°C to 33.9°C) at 72 hours to 38.0°C (37.5°C to 38.1°C) at 114 hours (P <0.001). In general, the cytokines and chemokines remained stable during hypothermia and decreased during rewarming, whereas complement activation was suppressed during the whole hypothermia period and increased modestly during rewarming.
Prolonged hypothermia may blunt the inflammatory response after rewarming in patients after cardiac arrest. Complement activation was low during the whole hypothermia period, indicating that complement activation is also highly temperature-sensitive in vivo. Because inflammation is a strong mediator of secondary brain injury, a blunted proinflammatory response after rewarming may be beneficial.
全身缺血再灌注会引发全身炎症反应。在本研究中,我们分析了温度对心脏骤停后接受长时间轻度低温治疗患者炎症反应的影响。
10例无脉性电活动/心搏停止或长时间室颤后恢复自主循环的昏迷患者,在一所三级大学医院入院后接受72小时的轻度治疗性低温治疗。入院时以及12、24、36、48、72、96和114小时测量患者体温,并从动脉导管采集血样。检测促炎细胞因子白细胞介素6(IL-6)和抗炎细胞因子(IL-10)、趋化因子(IL-8和单核细胞趋化蛋白1)、细胞间黏附分子1以及补体激活产物(C1r-C1s-C1抑制剂、C4bc、C3bPBb、C3bc和末端补体复合物)。使用非参数数据的重复测量检验分析随时间的变化。采用邓恩多重比较检验比较各个时间点。
研究开始时的中位体温为34.3°C(33.4°C至35.2°C),并在32°C至34°C之间维持72小时。72小时后所有患者被动复温,从72小时时的(中位(四分位间距))33.7°C(33.1°C至33.9°C)升至114小时时的38.0°C(37.5°C至38.1°C)(P<0.001)。总体而言,细胞因子和趋化因子在低温期间保持稳定,复温期间下降,而补体激活在整个低温期受到抑制,复温期间略有增加。
长时间低温可能会减弱心脏骤停患者复温后的炎症反应。整个低温期补体激活水平较低,表明补体激活在体内也对温度高度敏感。由于炎症是继发性脑损伤的重要介质,复温后减弱的促炎反应可能有益。