Feigenson Keith A, Keane Brian P, Roché Matthew W, Silverstein Steven M
Rutgers, Robert Wood Johnson Medical School, Department of Psychiatry, 675 Hoes Lane, Piscataway, NJ 08854, USA; Albright College, 13th and Bern Streets, Reading, PA 19612-52345, USA.
Rutgers, Robert Wood Johnson Medical School, Department of Psychiatry, 675 Hoes Lane, Piscataway, NJ 08854, USA; Rutgers University Behavioral Health Care, 671 Hoes Lane, Piscataway, NJ 08855, USA; Center for Cognitive Science, Rutgers, The State University of New Jersey, 152 Frelinghuysen Road, Piscataway, NJ 08854, USA.
Schizophr Res. 2014 Nov;159(2-3):515-20. doi: 10.1016/j.schres.2014.09.028. Epub 2014 Oct 11.
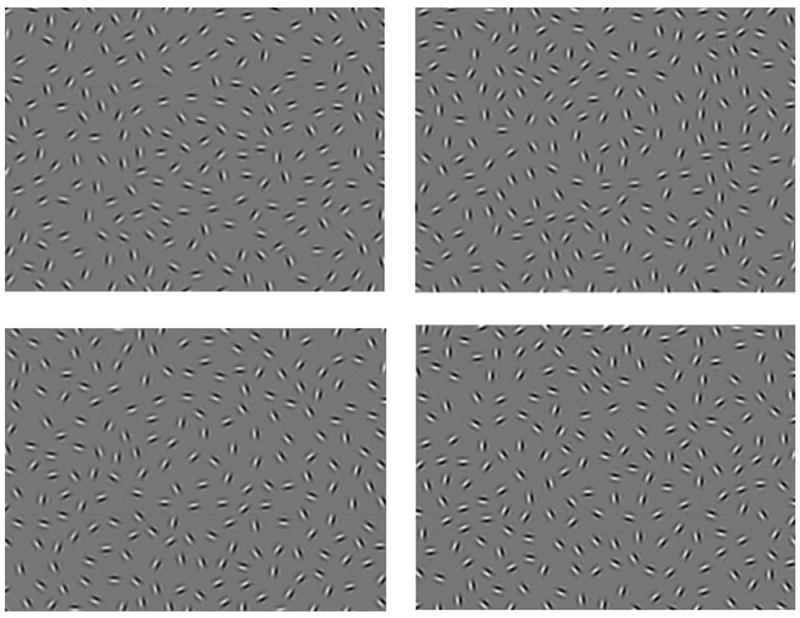
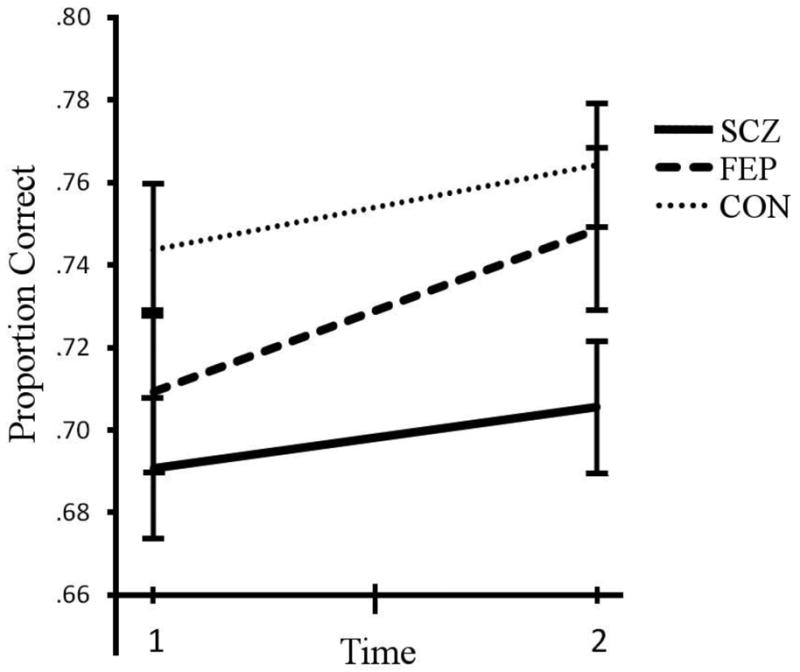
Contour integration is a fundamental visual process that recovers object structure by representing spatially separated edge elements as a continuous contour or shape boundary. Clinically stable persons with schizophrenia have repeatedly been shown to be impaired at contour integration but it is unclear whether this process varies with clinical state or whether it arises as early as the first episode of psychosis. To consider these issues, we administered a contour integration test to persons with chronic schizophrenia and to those with a first episode of psychosis. The test was administered twice-once at admission to short term psychiatric hospitalization and once again at discharge. A well-matched healthy control group was also tested across the same time points. We found that contour integration performance improved to the same degree in all groups over time, indicating that there were no recovery effects over and above normal practice effects. Moreover, the schizophrenia group demonstrated poorer contour integration than the control group and the first episode group exhibited intermediate performance that could not be distinguished from the other groups. These results suggest that contour integration ability does not vary as a function of short-term changes in clinical state, and that it may become further impaired with an increased number of psychotic episodes.
轮廓整合是一种基本的视觉过程,它通过将空间上分离的边缘元素表示为连续的轮廓或形状边界来恢复物体结构。反复研究表明,临床症状稳定的精神分裂症患者在轮廓整合方面存在缺陷,但尚不清楚这一过程是否随临床状态而变化,或者是否早在精神病发作的首次发作时就已出现。为了探讨这些问题,我们对慢性精神分裂症患者和首次发作精神病患者进行了轮廓整合测试。该测试在短期精神科住院入院时进行了一次,出院时又进行了一次。一个匹配良好的健康对照组也在相同的时间点进行了测试。我们发现,随着时间的推移,所有组的轮廓整合表现都有相同程度的提高,这表明除了正常的练习效果之外,不存在恢复效应。此外,精神分裂症组的轮廓整合能力比对照组差,首次发作组的表现介于两者之间,无法与其他组区分开来。这些结果表明,轮廓整合能力不会随着临床状态的短期变化而变化,并且可能随着精神病发作次数的增加而进一步受损。