Gurleyik Emin
Department of Surgery, Duzce University, Medical Faculty, Duzce, Turkey.
N Am J Med Sci. 2014 Sep;6(9):445-9. doi: 10.4103/1947-2714.141630.
Anatomical variations of the recurrent laryngeal nerve (RLN) such as extralaryngeal terminal bifurcation is an important risk for its motor function.
The objective is to study surgical anatomy of bilateral bifurcation of the RLNs in order to decrease risk of vocal cord palsy in patients with bifurcated nerves.
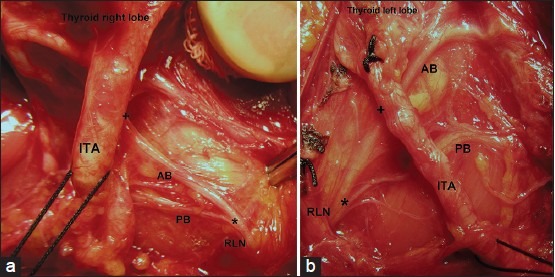
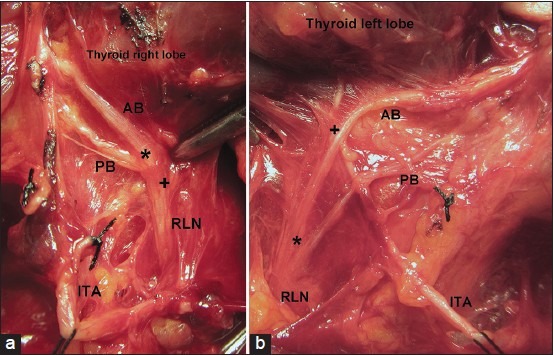
Surgical anatomy including terminal bifurcation was established in 292 RLNs of 146 patients. We included patients with bilateral bifurcation of RLN in this study. Based on two anatomical landmarks (nerve-artery crossing and laryngeal entry), the cervical course of RLN was classified in four segments: Pre-arterial, arterial, post-arterial and pre-laryngeal. According to these segments, bifurcation point locations along the cervical course of RLNs were compared between both sides in bilateral cases.
RLNs were exposed throughout their entire courses. Seventy (48%) patients had bifurcated RLNs. We identified terminal bifurcation in 90 (31%) of 292 RLNs along the cervical course. Bilateral bifurcation was observed in 20 (28.6%) patients with bifurcated RLNs. Bifurcation points were located on arterial and post-arterial segments in 37.5% and 32.5% of cases, respectively. Pre-arterial and pre-laryngeal segments contained bifurcations in 15% of cases. Comparison of both sides indicated that bifurcation points were similar in 5 (25%) and different in 15 (75%) patients with bilateral bifurcation. Permanent nerve injury did not occur in this series.
Bilateral bifurcation of both RLNs was observed in approximately 30% of patients with extralaryngeal bifurcation which is a common anatomical variation. Bifurcation occurred in different segments along cervical course of RLN. Bifurcation point locations differed between both sides in the majority of bilateral cases. Increasing surgeons' awareness of this variation may lead to safely exposing bifurcated nerves and prevent the injury to extralaryngeal terminal branches of RLN.
喉返神经(RLN)的解剖变异,如喉外终末分支,对其运动功能是一个重要风险。
目的是研究双侧喉返神经分支的手术解剖结构,以降低神经分支患者声带麻痹的风险。
在146例患者的292条喉返神经中建立了包括终末分支的手术解剖结构。本研究纳入了双侧喉返神经分支的患者。基于两个解剖标志(神经-动脉交叉和喉入口),喉返神经的颈部走行分为四段:动脉前、动脉段、动脉后和喉前。根据这些段,比较双侧病例中喉返神经颈部走行上的分支点位置。
喉返神经全程均被暴露。70例(48%)患者有喉返神经分支。在292条喉返神经的颈部走行中,我们在90条(31%)中发现了终末分支。在20例(28.6%)有喉返神经分支的患者中观察到双侧分支。分别有37.5%和32.5%的病例中,分支点位于动脉段和动脉后段。动脉前段和喉前段在15%的病例中有分支。双侧比较表明,在5例(25%)双侧分支患者中,分支点相似,在15例(75%)中不同。本系列中未发生永久性神经损伤。
在大约30%有喉外分支的患者中观察到双侧喉返神经分支,这是一种常见的解剖变异。分支发生在喉返神经颈部走行的不同段。在大多数双侧病例中,双侧分支点位置不同。提高外科医生对这种变异的认识可能有助于安全暴露分支神经,并防止损伤喉返神经的喉外终末分支。