Richards David A, Ross Sarah, Robens Sarah, Borglin Gunilla
University of Exeter Medical School, Haighton Building, St Luke's Campus, Heavitree Road, Exeter EX1 2 LU, UK.
Trials. 2014 Oct 16;15:398. doi: 10.1186/1745-6215-15-398.
The 'cohort multiple Randomised Controlled Trial' (cmRCT) design has been proposed as a potential solution to poor recruitment into clinical trials. The design randomly selects participants eligible for experimental treatments from a pre-enrolled cohort of patients, recruiting participants to multiple trials from a single cohort. Controls remain unaware of their participation in specific trials.
We undertook a mixed methods study to determine the ethical acceptability, the proportion of patients in a routine service consenting to cohort participation, the proportion of these who would consent to being hypothetically randomly selected to receive new treatments, and the views of clinicians on the acceptability of the design. We submitted our cmRCT design for ethical review and recruited participants from people with anxiety and depression attending a community mental health service of twenty-one clinicians. We recorded the proportion of patients who were offered participation in the DiReCT study and the proportion that consented to researcher contact, medical record sharing, and who accepted to be randomly allocated to active treatment procedures in future hypothetical unspecified clinical trials. We used a thematic framework analysis to analyse clinician interviews.
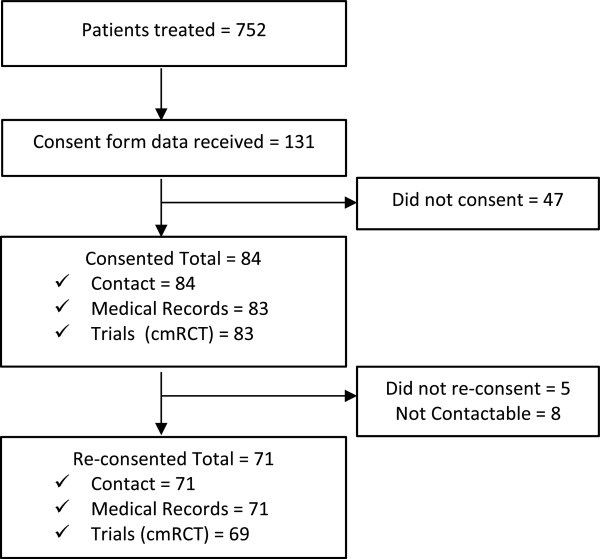
We obtained a favourable ethical opinion from the UK Health Research Authority. Clinicians approached 131/752 (17%) potentially eligible participants for consent. Of these 131, 84 (64%) initially consented to be contacted by a researcher and all but one consented to being randomised into future trials. We confirmed consent for 71 (54%) of participants approached by clinicians, of whom 69 (53%) consented to being randomised into hypothetical future trials, 9% (69/752) of all potentially eligible patients. The interviewed clinicians described issues impacting on their ability to recruit participants in terms of clinical concerns for patient wellbeing, work pressure, their views of both general research and the specific DiReCT study, and how they viewed patients' responses to being offered participation in the study.
The cmRCT system offers the potential to improve the recruitment into clinical trials and is acceptable ethically and to many patients. Overcoming the multiple factors driving the difficulties clinicians experience in patient recruitment is likely to require the application of significant implementation science-informed effort.
“队列多重随机对照试验”(cmRCT)设计被提议作为解决临床试验招募困难的一种潜在方案。该设计从预先登记的患者队列中随机选择符合实验性治疗条件的参与者,从单个队列中招募参与者参与多项试验。对照组患者并不知晓自己参与了特定试验。
我们开展了一项混合方法研究,以确定其伦理可接受性、常规服务中同意参与队列研究的患者比例、其中同意被假设随机选择接受新治疗的患者比例,以及临床医生对该设计可接受性的看法。我们将cmRCT设计提交进行伦理审查,并从参加由21名临床医生提供服务的社区心理健康服务机构的焦虑和抑郁患者中招募参与者。我们记录了被邀请参与直接比较治疗(DiReCT)研究的患者比例,以及同意研究者联系、共享病历并接受在未来假设的未明确临床试验中被随机分配至积极治疗程序的患者比例。我们使用主题框架分析法对临床医生访谈进行分析。
我们获得了英国健康研究管理局的正面伦理意见。临床医生向131/752(17%)名潜在符合条件的参与者寻求同意。在这131名参与者中,84名(64%)最初同意接受研究者联系,除一人外均同意被随机分配至未来试验。我们确认了临床医生邀请的71名(54%)参与者的同意,其中69名(53%)同意被随机分配至假设的未来试验,占所有潜在符合条件患者的9%(69/752)。接受访谈的临床医生描述了在招募参与者方面影响其能力的问题,涉及对患者福祉的临床担忧、工作压力、他们对一般研究和特定DiReCT研究的看法,以及他们对患者对参与研究邀请的反应的看法。
cmRCT系统有可能改善临床试验的招募情况,在伦理上以及对许多患者来说都是可接受的。克服推动临床医生在患者招募中遇到困难的多种因素,可能需要运用大量基于实施科学的努力。