Kumar G Anil, Dandona Rakhi, Chaman Priyanka, Singh Priyanka, Dandona Lalit
Public Health Foundation of India, Plot 47, Sector 44, Gurgaon 122002National Capital Region, India.
BMC Pregnancy Childbirth. 2014 Oct 17;14:357. doi: 10.1186/1471-2393-14-357.
A substantial reduction in neonatal deaths is required in India to meet the Millennium Development Goal of a two-thirds reduction in child mortality by 2015. We report neonatal mortality estimates and utilisation of maternal care in the Indian state of Bihar.
A representative population-based sample of 14,293 women who had a live birth in the last 12 months based on multistage sampling from all 38 districts of Bihar was selected for interview in early 2012. We estimated neonatal mortality rate and its associations using multiple logistic regression, assessed maternal care coverage and its inequality by wealth index, and retention of mothers in the health system for the full sequence of maternal care services.
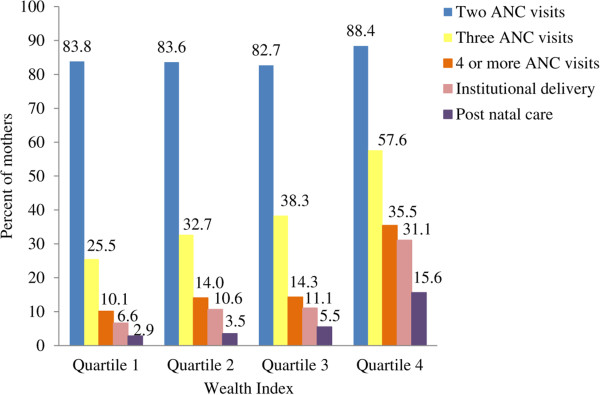
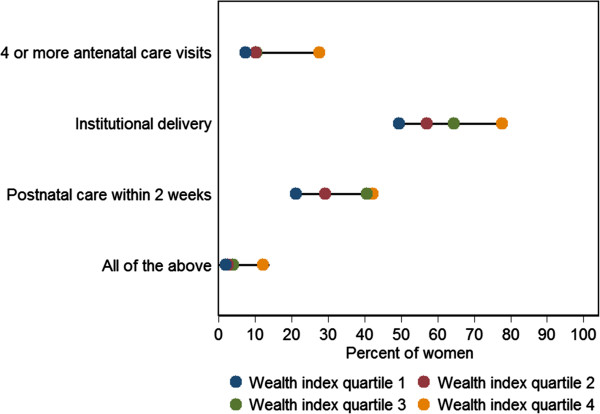
Neonatal mortality rate for Bihar was 32.2 (95% confidence interval [CI] 27.6-36.8) per 1,000 live births. Postnatal care related variables were significantly associated with neonatal deaths - no delayed bathing of new born (odds ratio [OR] 3.45, 95% CI 2.47-4.81) and no kangaroo care immediately after birth (OR 2.20, 95% CI 1.49-3.25). History of maternal complications and delivery in a private sector health facility had nearly twice the odds of neonatal death; the latter was driven by the very high neonatal mortality associated with private facility delivery in the lower two wealth index quartiles. A pattern of mass deprivation was seen for coverage of 4 or more ANC visits, health facility delivery and postnatal care for the same woman, with only 5.2% of women receiving this overall; this coverage was low for the highest wealth index quartile as well at 12.2%. Coverage of 4 or more ANC visits was 7.4% and 27.7% in the lowest and the highest wealth quartiles, respectively. Giving birth in a health facility was reported by 49.5% of women in the lowest wealth index quartile and by 77.7% in the highest quartile. Only 21.2% women reported post-natal care within 2 weeks of delivery in the lowest wealth index quartile, and 42.2% in the highest quartile.
Neonatal mortality continues to be relatively high in Bihar, and the utilization of maternal care very low and inequitable. Interventions need to address these deficiencies.
为实现到2015年将儿童死亡率降低三分之二的千年发展目标,印度需要大幅降低新生儿死亡率。我们报告了印度比哈尔邦的新生儿死亡率估计以及孕产妇保健的利用情况。
2012年初,通过对比哈尔邦所有38个区进行多阶段抽样,选取了14293名在过去12个月内有活产的具有代表性的基于人群的妇女样本进行访谈。我们使用多重逻辑回归估计新生儿死亡率及其关联,通过财富指数评估孕产妇保健覆盖率及其不平等情况,以及母亲在整个孕产妇保健服务序列中在卫生系统中的留存情况。
比哈尔邦的新生儿死亡率为每1000例活产32.2例(95%置信区间[CI] 27.6 - 36.8)。产后护理相关变量与新生儿死亡显著相关——新生儿无延迟沐浴(优势比[OR] 3.45,95% CI 2.47 - 4.81)以及出生后无袋鼠式护理(OR 2.20,95% CI 1.49 - 3.25)。孕产妇并发症史以及在私立部门卫生设施分娩的新生儿死亡几率几乎高出一倍;后者是由较低的两个财富指数四分位数中与私立机构分娩相关的极高新生儿死亡率所驱动。对于同一名妇女,接受4次或更多次产前检查、在卫生设施分娩和产后护理的覆盖率呈现出大规模匮乏的模式,只有5.2%的妇女能全部获得这些服务;在最高财富指数四分位数中,这一覆盖率也较低,为12.2%。在最低和最高财富四分位数中,接受4次或更多次产前检查的覆盖率分别为7.4%和27.7%。在最低财富指数四分位数中,49.5%的妇女报告在卫生设施分娩,在最高四分位数中为77.7%。在最低财富指数四分位数中,只有21.2%的妇女报告在分娩后2周内接受了产后护理,在最高四分位数中为42.2%。
比哈尔邦的新生儿死亡率仍然相对较高,孕产妇保健的利用率非常低且不平等。需要采取干预措施来解决这些不足。