Kenyon Chris Richard, Osbak Kara, Buyze Jozefien
Sexually Transmitted Infections, HIV/STI Unit, Institute of Tropical Medicine, Antwerp, Belgium ; Division of Infectious Diseases and HIV Medicine, University of Cape Town, Anzio Road, Observatory 7700, South Africa.
HIV/STI Unit, Institute of Tropical Medicine, Antwerp, Belgium.
Interdiscip Perspect Infect Dis. 2014;2014:284317. doi: 10.1155/2014/284317. Epub 2014 Sep 24.
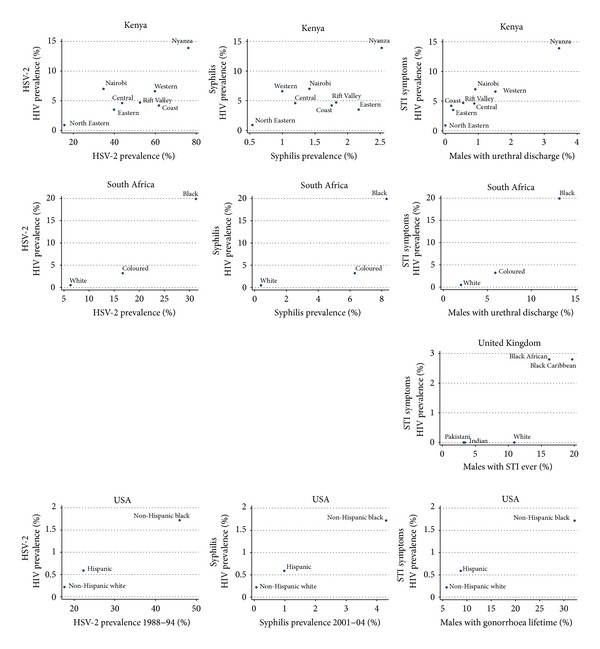
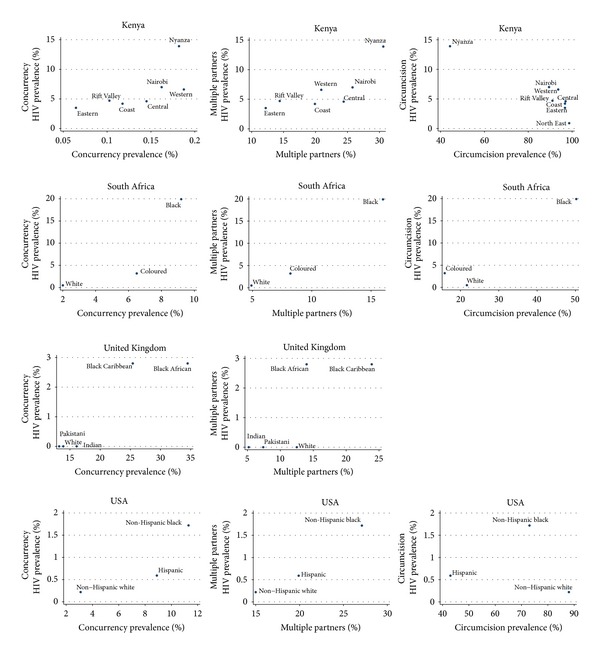
Background. This paper investigates two issues: do ethnic/racial groups with high HIV prevalences also have higher prevalences of other STIs? and is HIV prevalence by ethnic group correlated with the prevalence of circumcision, concurrency, or having more than one partner in the preceding year? Methods. We used Spearman's correlation to estimate the association between the prevalence of HIV per ethnic/racial group and HSV-2, syphilis, symptoms of an STI, having more than one partner in the past year, concurrency, and circumcision in Kenya, South Africa, the United Kingdom, and the United States. Results. We found that in each country HSV-2, syphilis, and symptomatic STIs were positively correlated with HIV prevalence (HSV-2: Kenya rho = 0.50, P = 0.207; South Africa rho-1, P = 0.000; USA rho-1, P = 0.000, Syphilis: Kenya rho = 0.33, P = 0.420; South Africa rho-1, P = 0.000; USA rho-1, P = 0.000, and STI symptoms: Kenya rho = 0.92, P = 0.001; South Africa rho-1, P = 0.000; UK rho = 0.87, P = 0.058; USA rho-1, P = 0.000). The prevalence of circumcision was only negatively associated with HIV prevalence in Kenya. Both having more than one partner in the previous year and concurrency were positively associated with HIV prevalence in all countries (concurrency: Kenya rho = 0.79, P = 0.036; South Africa rho-1, P = 0.000; UK 0.87, P = 0.058; USA rho-1, P = 0.000 and multiple partners: Kenya rho = 0.82, P = 0.023; South Africa rho-1, P = 0.000; UK rho = 0.87, P = 0.058; USA rho-1, P = 0.000). Not all associations were statistically significant. Conclusion. Further attention needs to be directed to what determines higher rates of partner change and concurrency in communities with high STI prevalence.
背景。本文研究两个问题:艾滋病毒高流行率的族裔/种族群体是否也有其他性传播感染的较高流行率?以及按族裔划分的艾滋病毒流行率与包皮环切率、同时性伴侣关系或前一年有多个性伴侣的情况是否相关?方法。我们使用斯皮尔曼相关性来估计肯尼亚、南非、英国和美国每个族裔/种族群体的艾滋病毒流行率与单纯疱疹病毒2型(HSV - 2)、梅毒、性传播感染症状、过去一年有多个性伴侣、同时性伴侣关系以及包皮环切率之间的关联。结果。我们发现,在每个国家,HSV - 2、梅毒和有症状的性传播感染与艾滋病毒流行率呈正相关(HSV - 2:肯尼亚,相关系数rho = 0.50,P = 0.207;南非,rho = 1,P = 0.000;美国,rho = 1,P = 0.000;梅毒:肯尼亚,rho = 0.33,P = 0.420;南非,rho = 1,P = 0.000;美国,rho = 1,P = 0.000;性传播感染症状:肯尼亚,rho = 0.92,P = 0.001;南非,rho = 1,P = 0.000;英国,rho = 0.87,P = 0.058;美国,rho = 1,P = 0.000)。仅在肯尼亚,包皮环切率与艾滋病毒流行率呈负相关。前一年有多个性伴侣和同时性伴侣关系在所有国家都与艾滋病毒流行率呈正相关(同时性伴侣关系:肯尼亚,rho = 0.79,P = 0.036;南非,rho = 1,P = 0.000;英国,rho = 0.87,P = 0.058;美国,rho = 1,P = 0.000;多个性伴侣:肯尼亚,rho = 0.82,P = 0.023;南非,rho = 1,P = 0.000;英国,rho = 0.87,P = 0.058;美国,rho = 1,P = 0.000)。并非所有关联都具有统计学意义。结论。需要进一步关注是什么因素导致性传播感染高流行社区中更高的性伴侣更换率和同时性伴侣关系发生率。