Battey Thomas W K, Karki Mahima, Singhal Aneesh B, Wu Ona, Sadaghiani Saloomeh, Campbell Bruce C V, Davis Stephen M, Donnan Geoffrey A, Sheth Kevin N, Kimberly W Taylor
From the Center for Human Genetic Research (T.W.K.B., M.K., W.T.K.), Division of Neurocritical Care and Emergency Neurology (T.W.K.B., M.K., W.T.K.), J. Philip Kistler Stroke Research Center (T.W.K.B., M.K., A.B.S., O.W., S.S., W.T.K.), and Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology (O.W.), Massachusetts General Hospital, Boston; Department of Radiology, Royal Melbourne Hospital, Parkville, Victoria, Australia (B.C.V.C., S.M.D.); Florey Institute of Neuroscience and Mental Health, University of Melbourne, Parkville, Victoria, Australia (B.C.V.C., G.A.D.); and Division of Neurocritical Care and Emergency Neurology, Yale New Haven Hospital, CT (K.N.S.).
Stroke. 2014 Dec;45(12):3643-8. doi: 10.1161/STROKEAHA.114.006884. Epub 2014 Oct 21.
In malignant infarction, brain edema leads to secondary neurological deterioration and poor outcome. We sought to determine whether swelling is associated with outcome in smaller volume strokes.
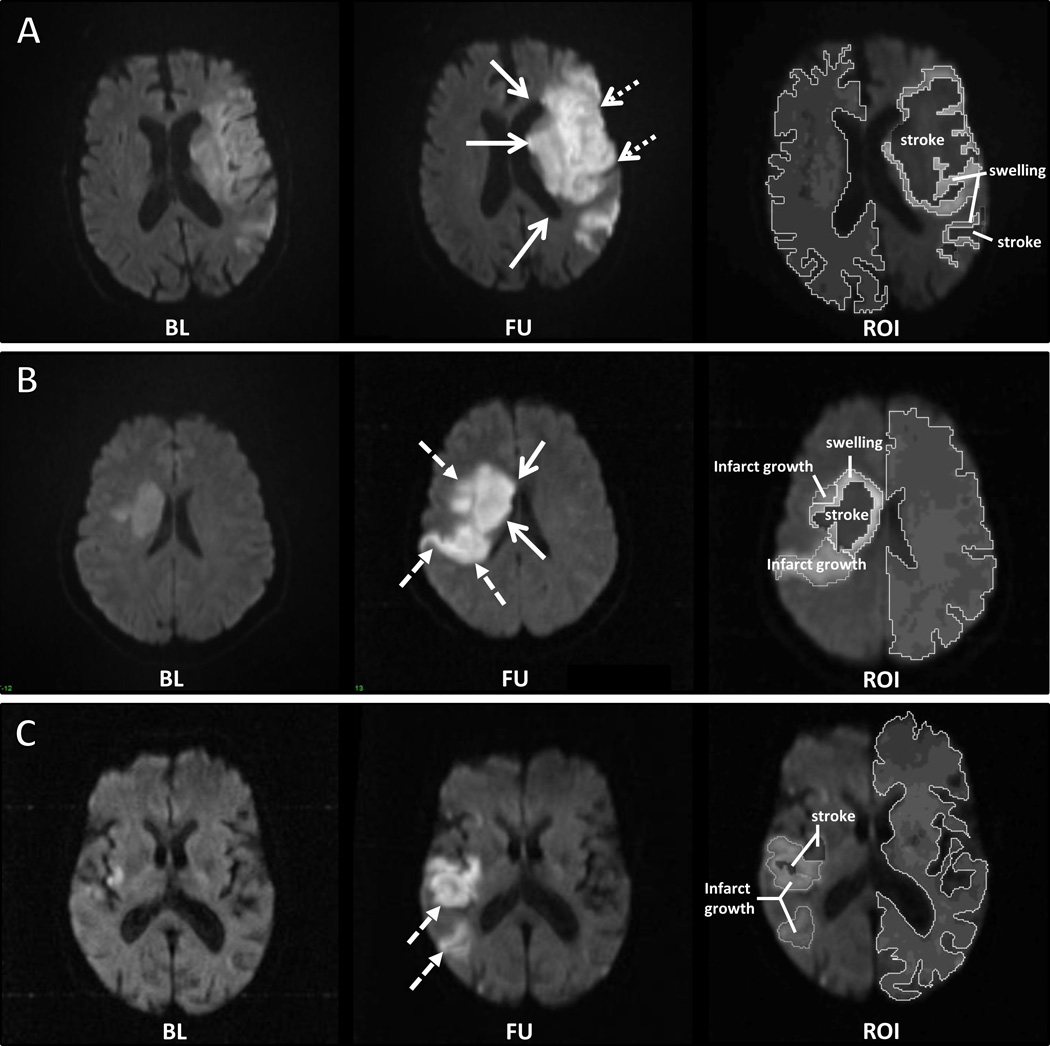
Two research cohorts of acute stroke subjects with serial brain MRI were analyzed. The categorical presence of swelling and infarct growth was assessed on diffusion-weighted imaging (DWI) by comparing baseline and follow-up scans. The increase in stroke volume (ΔDWI) was then subdivided into swelling and infarct growth volumes using region-of-interest analysis. The relationship of these imaging markers with outcome was evaluated in univariable and multivariable regression.
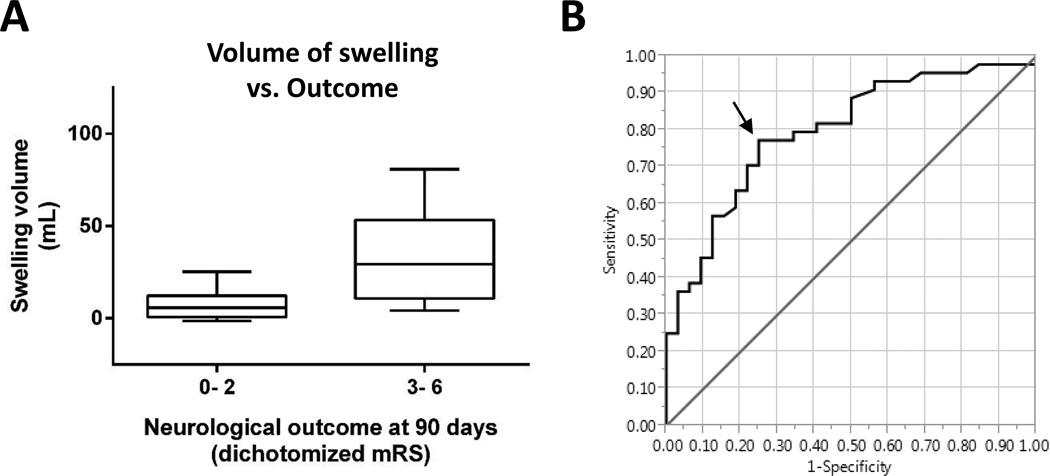
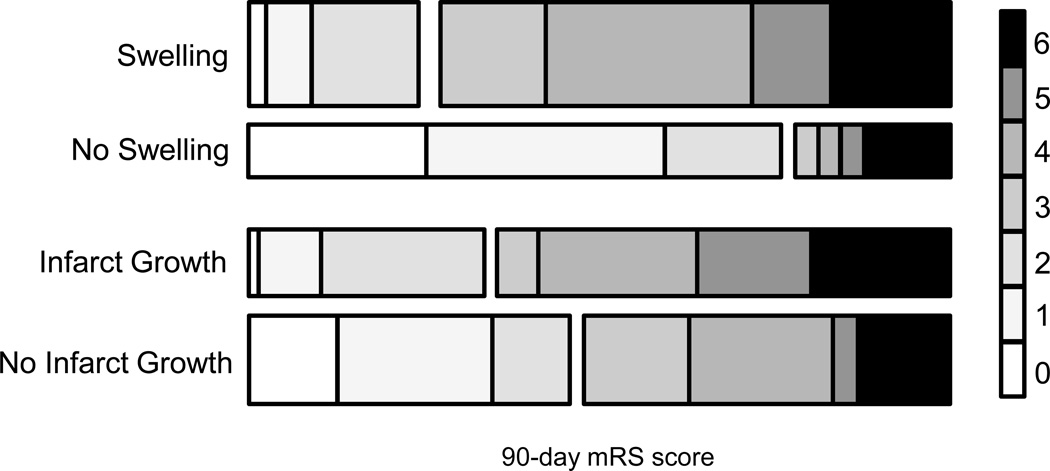
The presence of swelling independently predicted worse outcome after adjustment for age, National Institutes of Health Stroke Scale, admission glucose, and baseline DWI volume (odds ratio, 4.55; 95% confidence interval, 1.21-18.9; P<0.02). Volumetric analysis confirmed that ΔDWI was associated with outcome (odds ratio, 4.29; 95% confidence interval, 2.00-11.5; P<0.001). After partitioning ΔDWI into swelling and infarct growth volumetrically, swelling remained an independent predictor of poor outcome (odds ratio, 1.09; 95% confidence interval, 1.03-1.17; P<0.005). Larger infarct growth was also associated with poor outcome (odds ratio, 7.05; 95% confidence interval, 1.04-143; P<0.045), although small infarct growth was not. The severity of cytotoxic injury measured on apparent diffusion coefficient maps was associated with swelling, whereas the perfusion deficit volume was associated with infarct growth.
Swelling and infarct growth each contribute to total stroke lesion growth in the days after stroke. Swelling is an independent predictor of poor outcome, with a brain swelling volume of ≥11 mL identified as the threshold with greatest sensitivity and specificity for predicting poor outcome.
在恶性梗死中,脑水肿会导致继发性神经功能恶化及预后不良。我们试图确定在较小体积的卒中中,脑肿胀是否与预后相关。
对两个有系列脑部MRI检查的急性卒中受试者研究队列进行分析。通过比较基线和随访扫描,在扩散加权成像(DWI)上评估肿胀和梗死灶扩大的分类情况。然后使用感兴趣区分析将卒中体积增加量(ΔDWI)细分为肿胀和梗死灶扩大体积。在单变量和多变量回归中评估这些影像标志物与预后的关系。
在对年龄、美国国立卫生研究院卒中量表、入院血糖和基线DWI体积进行校正后,肿胀的存在独立预测了更差的预后(比值比,4.55;95%置信区间,1.21 - 18.9;P<0.02)。体积分析证实ΔDWI与预后相关(比值比,4.29;95%置信区间,2.00 - 11.5;P<0.001)。在将ΔDWI按体积细分为肿胀和梗死灶扩大后,肿胀仍然是预后不良的独立预测因素(比值比,1.09;95%置信区间,1.03 - 1.17;P<0.005)。更大的梗死灶扩大也与预后不良相关(比值比,7.05;95%置信区间,1.04 - 143;P<0.045),尽管小梗死灶扩大与预后不良无关。在表观扩散系数图上测量的细胞毒性损伤严重程度与肿胀相关,而灌注缺损体积与梗死灶扩大相关。
肿胀和梗死灶扩大均在卒中后数天内对总卒中病灶增长有影响。肿胀是预后不良的独立预测因素,脑肿胀体积≥11 mL被确定为预测预后不良具有最高敏感性和特异性的阈值。