Department of Cardiovascular Medicine, The Alfred Hospital, Commercial Road, Melbourne, VIC 3004 Australia ; Baker IDI Heart and Diabetes Institute, 75 Commercial Road, Melbourne, VIC 3004 Australia ; Department of Cardiovascular Medicine, The 1st Affiliated Hospital of Medical College, Xi'an Jiaotong University, Xi'an, 710061 China.
Department of Cardiovascular Medicine, The Alfred Hospital, Commercial Road, Melbourne, VIC 3004 Australia ; Baker IDI Heart and Diabetes Institute, 75 Commercial Road, Melbourne, VIC 3004 Australia.
J Inflamm (Lond). 2014 Oct 11;11(1):29. doi: 10.1186/s12950-014-0029-0. eCollection 2014.
Inflammation plays an important role in the pathogenesis of atherosclerosis. The link between rheumatoid arthritis (RA) and an increased risk of cardiovascular disease and mortality is well established; however, the association between inflammatory bowel disease (IBD) and cardiovascular risk is controversial. Arterial stiffness is both a marker and risk factor for atherosclerosis. Here we aimed to 1) compare circulating markers of inflammation and endothelial dysfunction, traditional cardiovascular risk factors, and arterial stiffness between RA and IBD to help to understand their different associations with cardiovascular disease; 2) assess the impacts of circulating markers of inflammation and endothelial dysfunction, and traditional risk factors on arterial stiffness.
Patients with RA (n = 43) and IBD (n = 42), and control subjects (n = 73) were recruited. Plasma inflammatory markers and von Willebrand factor (vWF) were measured by Multiplex assays or ELISA. Arterial stiffness was determined by brachial-ankle pulse wave velocity (baPWV) and ankle-brachial index (ABI) was measured. Framingham Risk Score (FRS) was calculated, and other traditional risk factors were also documented.
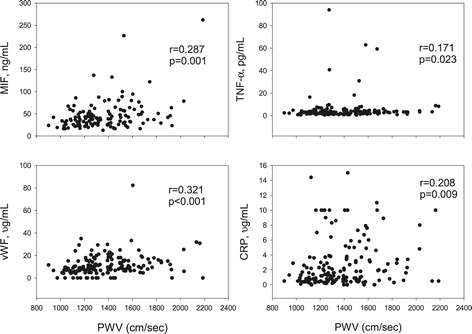
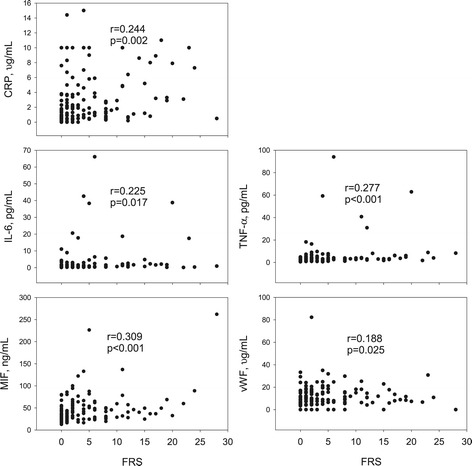
Plasma levels of several inflammatory markers and vWF were significantly but comparably elevated in RA and IBD compared with controls, except for a higher level of C-reactive protein (CRP) in RA than IBD. Compared to controls, FRS, body mass index, waist circumference, and triglycerides were increased in RA, but not in IBD. baPWV did not significantly differ among 3 groups, while ABI was modestly but significantly lower in IBD than controls. Circulating markers (macrophage migration inhibitory factor, tumour necrosis factor-α, CRP, and vWF) were significantly associated with baPWV. However, traditional risk factors (age, systolic blood pressure, body mass index, diabetes and triglycerides) were the parameters associated with baPWV in multiple regression analyses (overall r = 0.866, p < 0.001).
RA has a higher level of CRP and more pronounced traditional cardiovascular risk factors than IBD, which may contribute to the difference in their associations with cardiovascular disease and mortality. Traditional risk factors, rather than inflammation markers, are major predictors of arterial stiffness even in subjects with inflammatory disorders. Our results point to the importance of modifying traditional risk factors in patients with inflammatory disorders.
炎症在动脉粥样硬化的发病机制中起重要作用。类风湿关节炎(RA)与心血管疾病风险增加和死亡率增加之间的联系已得到充分证实;然而,炎症性肠病(IBD)与心血管风险之间的关联仍存在争议。动脉僵硬度既是动脉粥样硬化的标志物又是其危险因素。在这里,我们旨在:1)比较 RA 和 IBD 之间循环炎症标志物和内皮功能障碍、传统心血管危险因素和动脉僵硬度,以帮助了解它们与心血管疾病的不同关联;2)评估循环炎症标志物和内皮功能障碍以及传统危险因素对动脉僵硬度的影响。
招募了 43 名 RA 患者、42 名 IBD 患者和 73 名对照者。通过多重分析或 ELISA 测量血浆炎症标志物和血管性血友病因子(vWF)。通过肱踝脉搏波速度(baPWV)测定动脉僵硬度,并测量踝臂指数(ABI)。计算 Framingham 风险评分(FRS),并记录其他传统危险因素。
与对照组相比,RA 和 IBD 患者的几种炎症标志物和 vWF 水平均显著升高,但程度相当,而 RA 患者的 C 反应蛋白(CRP)水平高于 IBD 患者。与对照组相比,RA 患者的 FRS、体重指数、腰围和甘油三酯升高,但 IBD 患者没有升高。3 组间 baPWV 无显著差异,而 IBD 患者的 ABI 略低于对照组。循环标志物(巨噬细胞移动抑制因子、肿瘤坏死因子-α、CRP 和 vWF)与 baPWV 显著相关。然而,在多元回归分析中,传统危险因素(年龄、收缩压、体重指数、糖尿病和甘油三酯)是与 baPWV 相关的参数(总体 r=0.866,p<0.001)。
RA 患者的 CRP 水平较高,且存在更明显的传统心血管危险因素,这可能导致其与心血管疾病和死亡率的关联存在差异。传统危险因素而非炎症标志物是动脉僵硬度的主要预测因素,即使在存在炎症性疾病的患者中也是如此。我们的研究结果表明,在炎症性疾病患者中,改变传统危险因素非常重要。