Frayne Susan M, Holmes Tyson H, Berg Eric, Goldstein Mary K, Berlowitz Dan R, Miller Donald R, Pogach Leonard M, Laungani Kaajal J, Lee Tina T, Moos Rudolf
Department of Veterans Affairs HSR&D Center for Innovation to Implementation (Ci2i), VA Palo Alto Health Care System, 795 Willow Road (152-MPD), Menlo Park, CA 94025, USA.
BMC Health Serv Res. 2014 Oct 22;14:458. doi: 10.1186/1472-6963-14-458.
Mental health condition (MHC) comorbidity is associated with lower intensity care in multiple clinical scenarios. However, little is known about the effect of MHC upon clinicians' decisions about intensifying antiglycemic medications in diabetic patients with poor glycemic control. We examined whether delay in intensification of antiglycemic medications in response to an elevated Hemoglobin A1c (HbA1c) value is longer for patients with MHC than for those without MHC, and whether any such effect varies by specific MHC type.
In this observational study of diabetic Veterans Health Administration (VA) patients on oral antiglycemics with poor glycemic control (HbA1c ≥8) (N =52,526) identified from national VA databases, we applied Cox regression analysis to examine time to intensification of antiglycemics after an elevated HbA1c value in 2003-2004, by MHC status.
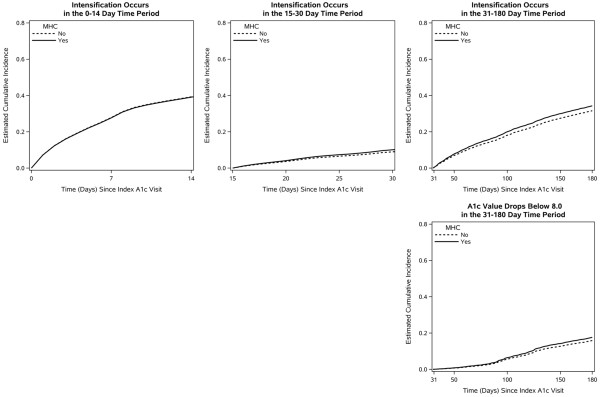
Those with MHC were no less likely to receive intensification: adjusted Hazard Ratio [95% CI] 0.99 [0.96-1.03], 1.13 [1.04-1.23], and 1.12 [1.07-1.18] at 0-14, 15-30 and 31-180 days, respectively. However, patients with substance use disorders were less likely than those without substance use disorders to receive intensification in the first two weeks following a high HbA1c, adjusted Hazard Ratio 0.89 [0.81-0.97], controlling for sex, age, medical comorbidity, other specific MHCs, and index HbA1c value.
For most MHCs, diabetic patients with MHC in the VA health care system do not appear to receive less aggressive antiglycemic management. However, the subgroup with substance use disorders does appear to have excess likelihood of non-intensification; interventions targeting this high risk subgroup merit attention.
在多种临床情况下,心理健康状况(MHC)合并症与较低强度的治疗相关。然而,关于MHC对临床医生针对血糖控制不佳的糖尿病患者强化降糖药物治疗决策的影响,我们知之甚少。我们研究了血糖控制不佳的糖尿病患者中,MHC患者相较于非MHC患者,对糖化血红蛋白(HbA1c)值升高做出反应时,强化降糖药物治疗的延迟是否更长,以及这种影响是否因特定的MHC类型而异。
在这项对从退伍军人健康管理局(VA)全国数据库中识别出的接受口服降糖药治疗且血糖控制不佳(HbA1c≥8)的糖尿病患者(N = 52,526)进行的观察性研究中,我们应用Cox回归分析,按MHC状态检查2003 - 2004年HbA1c值升高后强化降糖药物治疗的时间。
有MHC的患者接受强化治疗的可能性并不低:在0 - 14天、15 - 30天和31 - 180天的调整后风险比[95%置信区间]分别为0.99[0.96 - 1.03]、1.13[1.04 - 1.23]和1.12[1.07 - 1.18]。然而,在HbA1c升高后的前两周内,患有物质使用障碍的患者比没有物质使用障碍的患者接受强化治疗的可能性更低,调整后风险比为0.89[0.81 - 0.97],同时控制了性别、年龄、合并症、其他特定的MHC以及初始HbA1c值。
对于大多数MHC,在VA医疗系统中患有MHC的糖尿病患者似乎并未接受不那么积极的降糖管理。然而,患有物质使用障碍的亚组确实似乎有更高的不强化治疗可能性;针对这一高风险亚组所采取的干预措施值得关注。