Chang Tae Ik, Kim Yung Ly, Kim Hyungwoo, Ryu Geun Woo, Kang Ea Wha, Park Jung Tak, Yoo Tae-Hyun, Shin Sug Kyun, Kang Shin-Wook, Choi Kyu Hun, Han Dae Suk, Han Seung Hyeok
Department of Internal Medicine, NHIS Medical Center, Ilsan Hospital, Goyangshi, Gyeonggi-do, Republic of Korea.
Department of Internal Medicine, College of Medicine, Yonsei University, Seoul, Republic of Korea.
PLoS One. 2014 Oct 29;9(10):e111373. doi: 10.1371/journal.pone.0111373. eCollection 2014.
Hyponatremia is common in patients with chronic kidney disease and is associated with increased mortality in hemodialysis patients. However, few studies have addressed this issue in peritoneal dialysis (PD) patients.
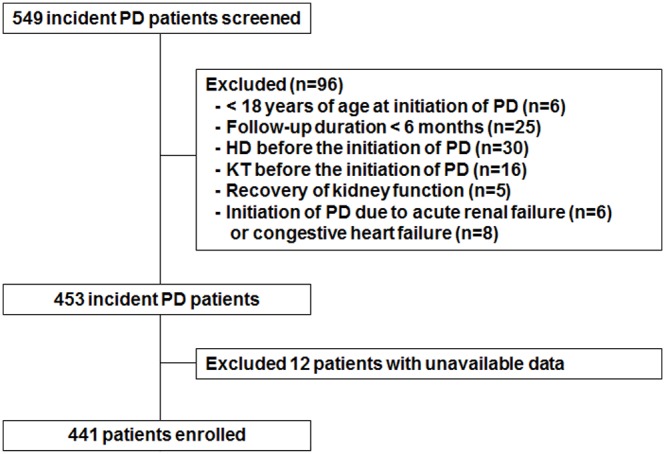
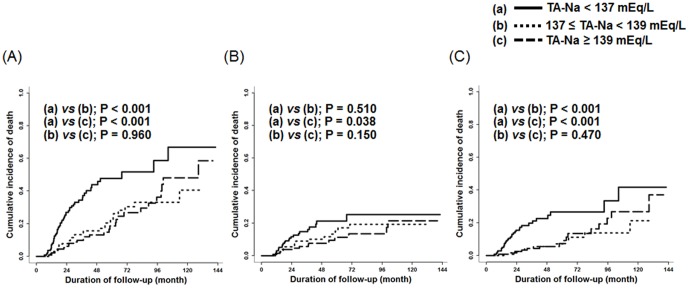
This prospective observational study included a total of 441 incident patients who started PD between January 2000 and December 2005. Using time-averaged serum sodium (TA-Na) levels, we aimed to investigate whether hyponatremia can predict mortality in these patients.
Among the baseline parameters, serum sodium level was positively associated with serum albumin (β = 0.145; p = 0.003) and residual renal function (RRF) (β = 0.130; p = 0.018) and inversely associated with PD ultrafiltration (β = -0.114; p = 0.024) in a multivariable linear regression analysis. During a median follow-up of 34.8 months, 149 deaths were recorded. All-cause death occurred in 81 (55.9%) patients in the lowest tertile compared to 37 (25.0%) and 31 (20.9%) patients in the middle and highest tertiles, respectively. After adjusting for multiple potentially confounding covariates, increased TA-Na level was associated with a significantly decreased risk of all-cause (HR per 1 mEq/L increase, 0.79; 95% CI, 0.73-0.86; p<0.001) and infection-related (HR per 1 mEq/L increase, 0.77; 95% CI, 0.70-0.85; p<0.001) deaths.
This study showed that hyponatremia is an independent predictor of mortality in PD patients. Nevertheless, whether correcting hyponatremia improves patient survival is unknown. Future interventional studies should address this question more appropriately.
低钠血症在慢性肾脏病患者中很常见,且与血液透析患者死亡率增加有关。然而,很少有研究探讨腹膜透析(PD)患者的这一问题。
这项前瞻性观察性研究共纳入了2000年1月至2005年12月开始进行PD的441例新发病例患者。我们旨在利用时间平均血清钠(TA-Na)水平来研究低钠血症是否能预测这些患者的死亡率。
在多变量线性回归分析中,血清钠水平在基线参数中与血清白蛋白呈正相关(β = 0.145;p = 0.003)和残余肾功能(RRF)呈正相关(β = 0.130;p = 0.018),与PD超滤呈负相关(β = -0.114;p = 0.024)。在中位随访34.8个月期间,记录到149例死亡。最低三分位数组中有81例(55.9%)患者发生全因死亡,而中间和最高三分位数组分别有37例(25.0%)和31例(20.9%)患者发生全因死亡。在调整了多个潜在混杂协变量后,TA-Na水平升高与全因死亡(每升高1 mEq/L的HR为0.79;95%CI为0.73 - 0.86;p<0.001)和感染相关死亡(每升高1 mEq/L的HR为0.77;95%CI为0.70 - 0.85;p<0.001)风险显著降低相关。
本研究表明低钠血症是PD患者死亡率的独立预测因素。然而,纠正低钠血症是否能改善患者生存尚不清楚。未来的干预性研究应更恰当地解决这个问题。