Suarez Alecha Javier, Amoza Pais Sonia, Batlle Marin Xavi, Oronoz Martinez Begoña, Balen Ribera Enrique, Yarnoz Irazabal Concepción
Departament of Surgery, Unit of Coloproctology, Complejo Hospitalario de Navarra, Pamplona, Spain.
Ann Coloproctol. 2014 Oct;30(5):216-21. doi: 10.3393/ac.2014.30.5.216. Epub 2014 Oct 28.
The role of surgery in the management of diverticular disease after an episode of acute diverticulitis (AD) managed in a conservative form is evolving. Age, number of episodes of AD, type of episode, and symptoms after the episodes are factors related to the need for elective surgery. The aim of this study is to evaluate the safety of conservative management and the risk factors for emergency surgery after a first episode of AD managed without surgery.
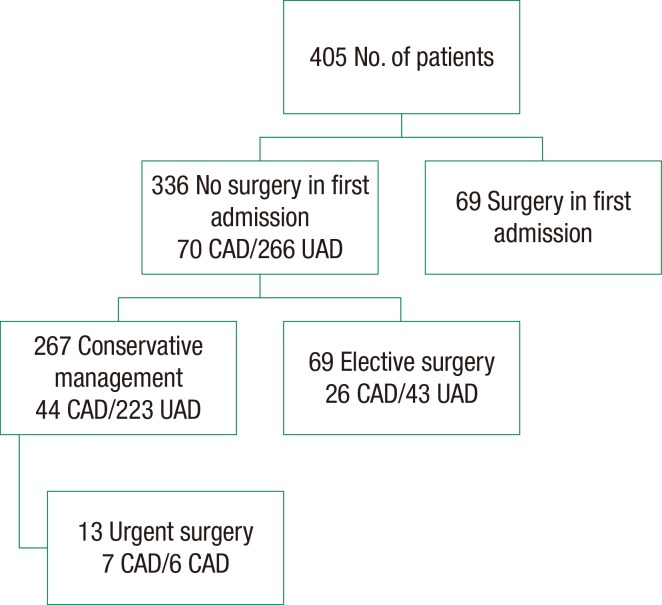
We retrospectively evaluated 405 patients diagnosed as having had a first episode of AD. Sixty-nine patients underwent emergency surgery on the first admission, and 69 patients had an elective operation in the follow-up (group A). The remaining 267 patients were managed initially without surgery (group B). Thirteen of these 267 patients needed a further urgent surgical procedure. Factors involved in the decision of elective surgery and the probability of emergency surgery after the first episode of AD managed without surgery were evaluated in relation to demographic factors, risk factors, presence of recurrences, and type of the first episode.
Patients, mean age was 62.7 years, 71 were aged less than 51, and 151 were males. The mean follow-up for patients with nonoperative management was 91.2 months. An elective operation was performed in 69 patients. Compared to patients in group B, those in group A more frequently had a first episode of complicated acute diverticulitis (CAD) (37.1% vs. 16.4%; P = 0.000) and were more likely to be smokers (46.3% vs. 19.3%; P = 0.000) and to suffer more than one episode of AD (42% vs. 26.9%; P = 0.027). Nonoperative management was chosen for 267 patients, but 13 patients needed an emergency operation later. In the multivariate analysis, we found a significant relation between the presence of CAD in the first episode and the need for emergency surgery. There were no differences in surgical mortality between the patients in the two groups, but patients treated with elective surgery had a higher rate of stoma than patients treated non-operatively (7.2% vs. 1.4%; P = 0.028); this difference was not observed in the subgroup of patients with CAD (15.3% vs. 6.8%; P = 0.458).
After an episode of AD, nonoperative management is safe because fewer than 5% of patients will need an emergent procedure in a subsequent attack of AD. A first episode of CAD is the only risk factor for emergency surgery in patients managed conservatively.
在以保守方式处理急性憩室炎(AD)发作后,手术在憩室病管理中的作用正在不断演变。年龄、AD发作次数、发作类型以及发作后的症状是与择期手术需求相关的因素。本研究的目的是评估保守治疗的安全性以及首次发作AD且未经手术治疗后急诊手术的危险因素。
我们回顾性评估了405例被诊断为首次发作AD的患者。69例患者在首次入院时接受了急诊手术,69例患者在随访期间接受了择期手术(A组)。其余267例患者最初未接受手术治疗(B组)。这267例患者中有13例需要进一步的紧急手术。针对人口统计学因素、危险因素、复发情况以及首次发作类型,评估了首次发作AD且未经手术治疗后择期手术决策和急诊手术可能性所涉及的因素。
患者平均年龄为62.7岁,71例年龄小于51岁,151例为男性。非手术治疗患者的平均随访时间为91.2个月。69例患者接受了择期手术。与B组患者相比,A组患者首次发作复杂急性憩室炎(CAD)的情况更常见(37.1%对16.4%;P = 0.000),更可能是吸烟者(46.3%对19.3%;P = 0.000),且AD发作次数更多(42%对26.9%;P = 0.027)。267例患者选择了非手术治疗,但13例患者后来需要急诊手术。在多变量分析中,我们发现首次发作CAD与急诊手术需求之间存在显著关联。两组患者的手术死亡率无差异,但接受择期手术的患者造口率高于非手术治疗的患者(7.2%对1.4%;P = 0.028);在CAD患者亚组中未观察到这种差异(15.3%对6.8%;P = 0.458)。
AD发作后,非手术治疗是安全的,因为在后续AD发作中需要紧急手术的患者不到5%。首次发作CAD是保守治疗患者急诊手术的唯一危险因素。