Zhang Qunhu, Yuan Zhen, Zhou Min, Liu Huan, Xu Yong, Ren Yongxin
Department of Orthopedics, The First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, Jiangsu, People's Republic of China.
BMC Musculoskelet Disord. 2014 Nov 5;15:367. doi: 10.1186/1471-2474-15-367.
We compared the perioperative results and complications associated with PLIF and TLIF, and collected evidence for choosing the better fusion method.
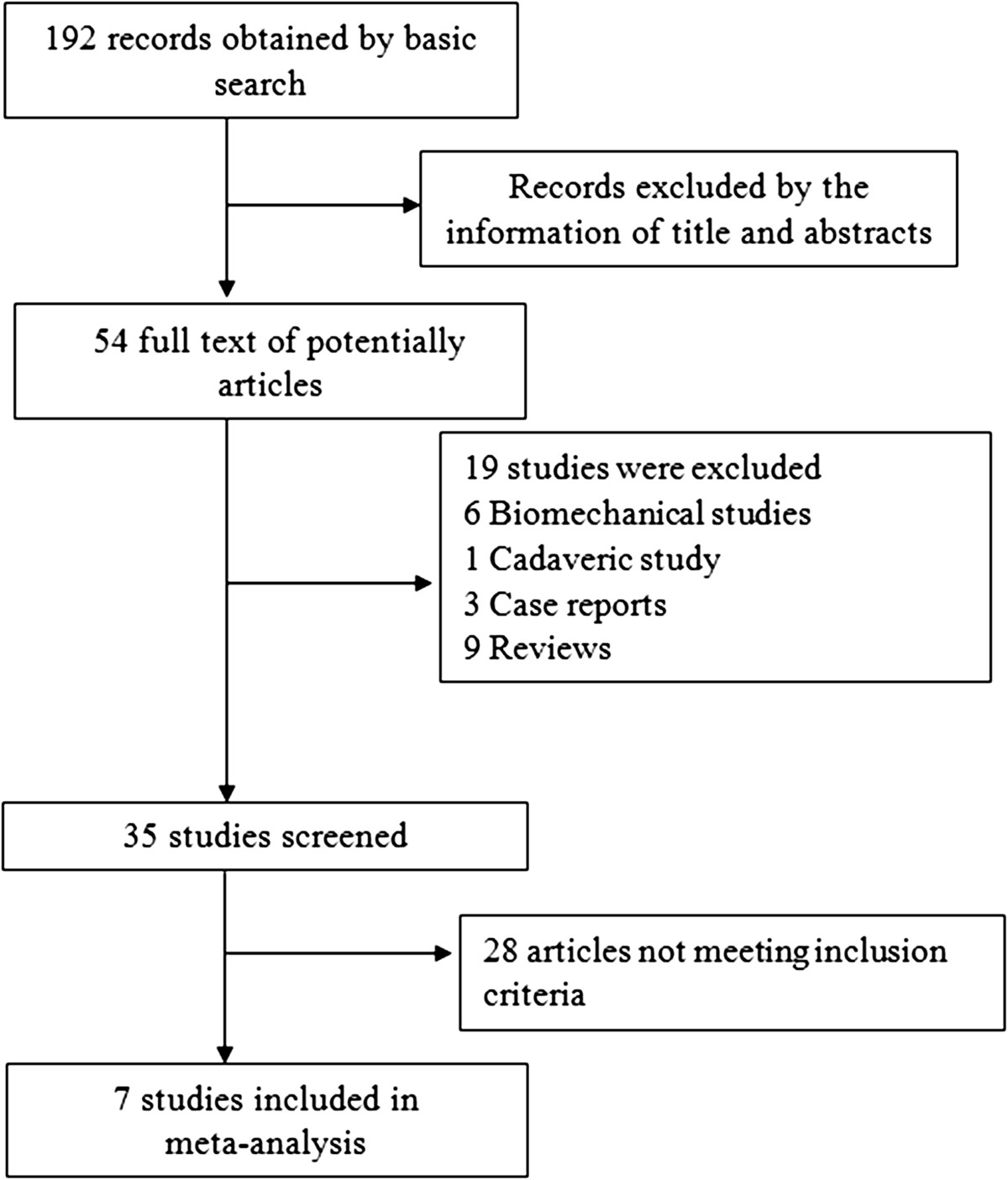
A literature survey of the MEDLINE and EMBASE databases identified 7 comparative observational studies that met our inclusion criteria. Checklists by Cowley were used to evaluate the risk of bias of the included studies. A database including patient demographic information, perioperative results, and complications was established. The summary odds ratio and weighed mean difference with 95% confidence interval were calculated with a random-effects model.
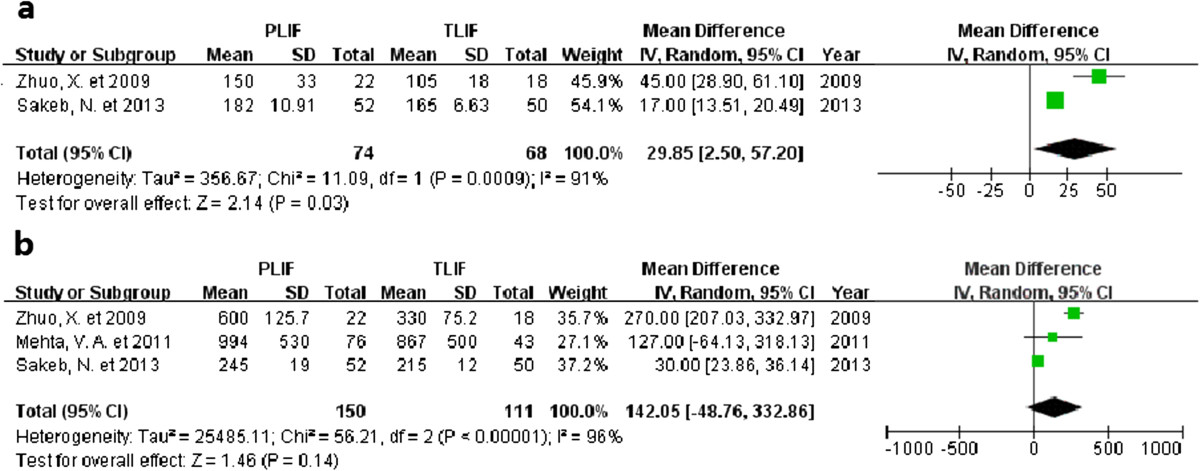
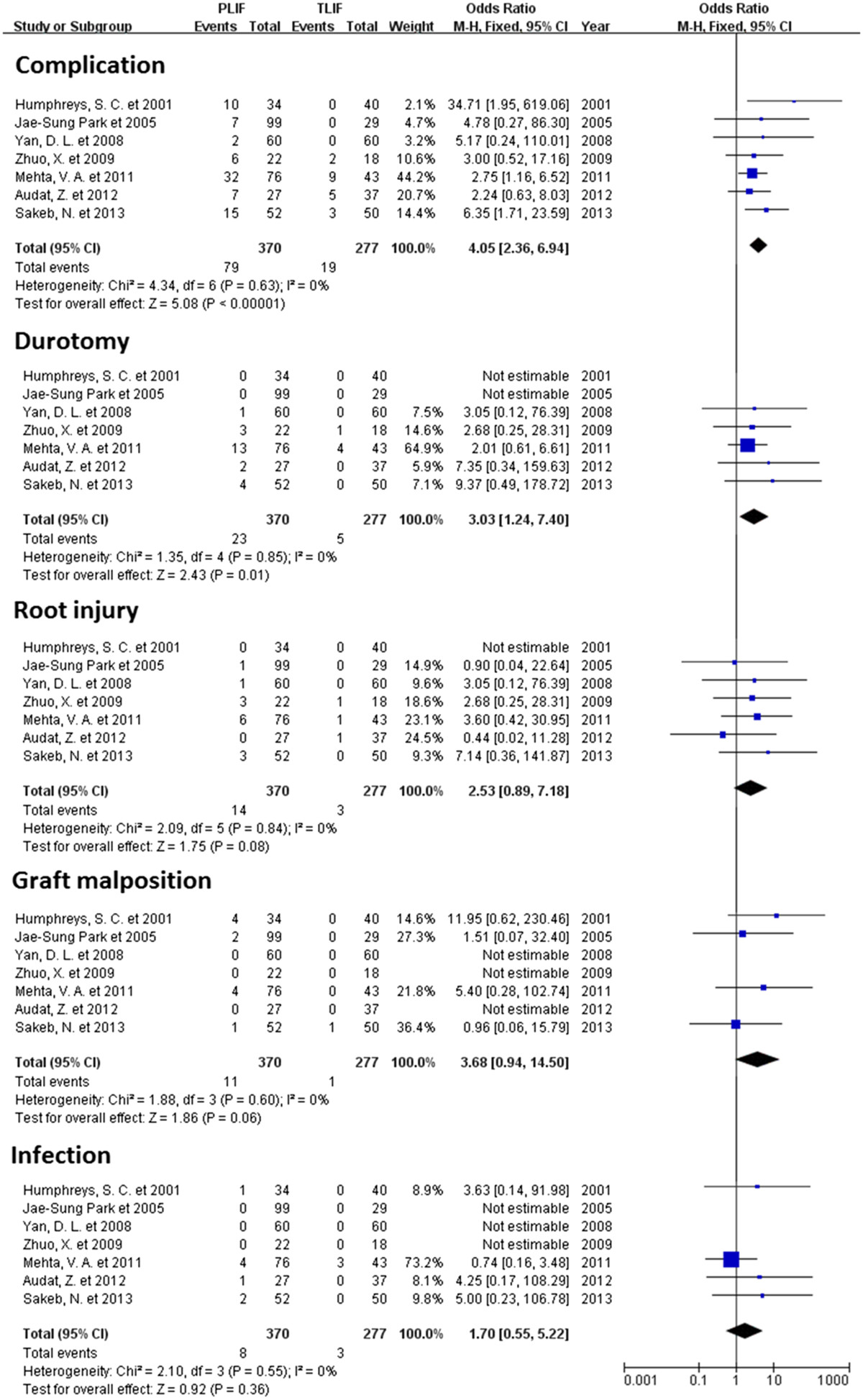
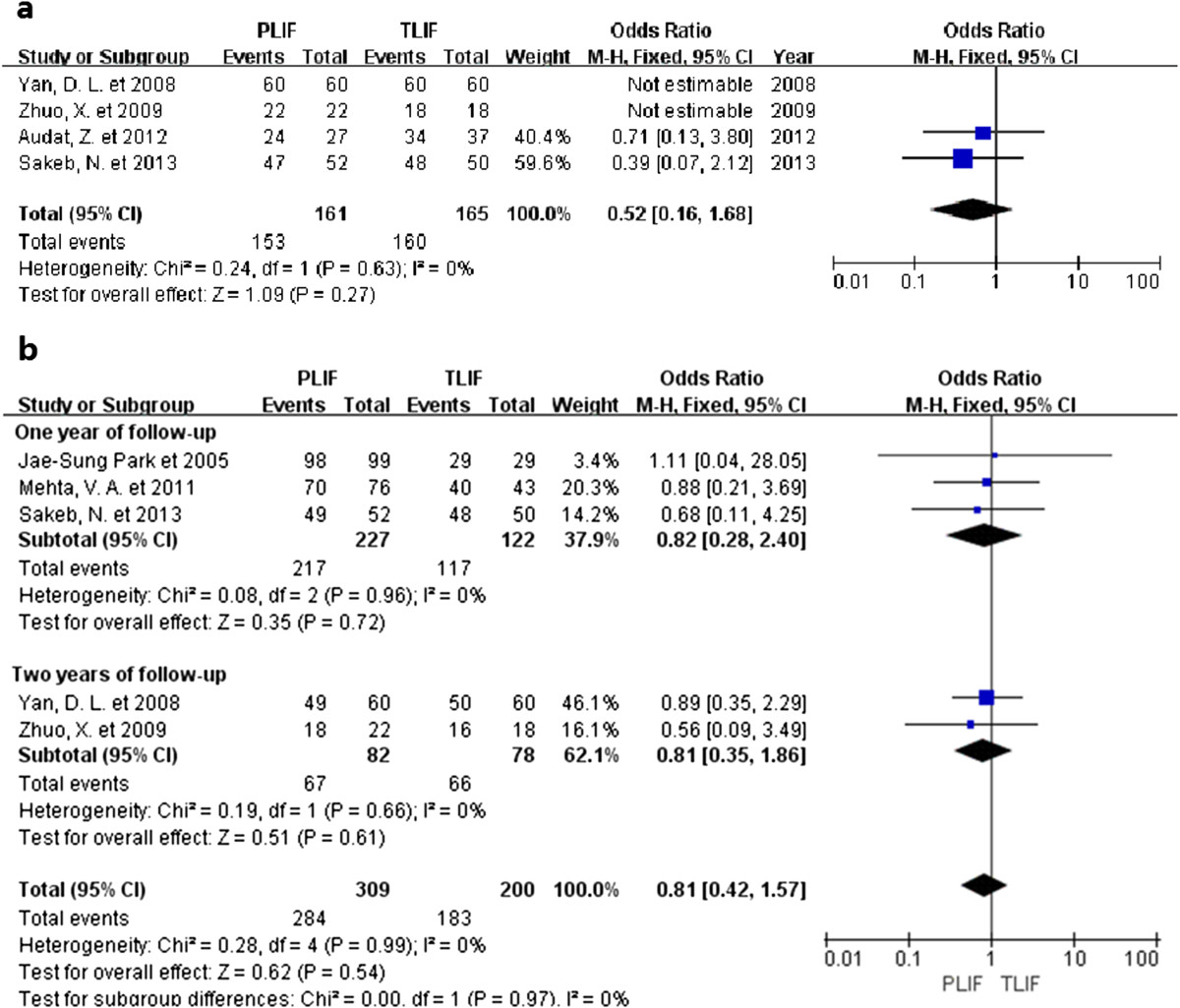
We found that PLIF had a higher complication rate (P <0.00001), and TLIF reduced the rate of durotomy (P = 0.01). No statistical difference was found between the two groups with regard to clinical satisfaction (P = 0.54), blood loss (P = 0.14), vertebral root injury (P = 0.08), graft malposition (P = 0.06), infection (P = 0.36), or rate of radiographic fusion (P = 0.27). The evidence indicated that PLIF required longer operative time (P = 0.03).
The evidence indicated that TLIF could reduce the complication rate and durotomy. Neither TLIP nor PLIF was found superior in terms of clinical satisfaction or radiographic fusion rate. PLIF might result in longer time in surgery.
我们比较了后路腰椎椎间融合术(PLIF)和经椎间孔腰椎椎间融合术(TLIF)的围手术期结果及并发症,为选择更好的融合方法收集证据。
对MEDLINE和EMBASE数据库进行文献检索,确定了7项符合我们纳入标准的比较观察性研究。使用考利清单评估纳入研究的偏倚风险。建立了一个包含患者人口统计学信息、围手术期结果和并发症的数据库。采用随机效应模型计算汇总比值比和加权平均差及其95%置信区间。
我们发现PLIF的并发症发生率更高(P<0.00001),TLIF降低了硬脊膜切开率(P=0.01)。两组在临床满意度(P=0.54)、失血量(P=0.14)、神经根损伤(P=0.08)、植骨位置不当(P=0.06)、感染(P=0.36)或影像学融合率(P=0.27)方面未发现统计学差异。证据表明PLIF需要更长的手术时间(P=0.03)。
证据表明TLIF可降低并发症发生率和硬脊膜切开率。在临床满意度或影像学融合率方面,未发现TLIF和PLIF有优势。PLIF可能导致手术时间更长。