Yang Jeong Hoon, Hahn Joo-Yong, Song Young Bin, Choi Seung-Hyuk, Choi Jin-Ho, Lee Sang Hoon, Jeong Myung-Ho, Choi Dong-Joo, Park Jong Seon, Park Hun Sik, Gwon Hyeon-Cheol
Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
BMJ. 2014 Nov 14;349:g6650. doi: 10.1136/bmj.g6650.
To investigate the association between treatment with an angiotensin receptor blocker and clinical outcomes in patients with ST segment elevation myocardial infarction with preserved left ventricular systolic function.
A prospective cohort study using data from a nationwide large scale registry.
53 hospitals involved in treatment of acute myocardial infarction in Korea.
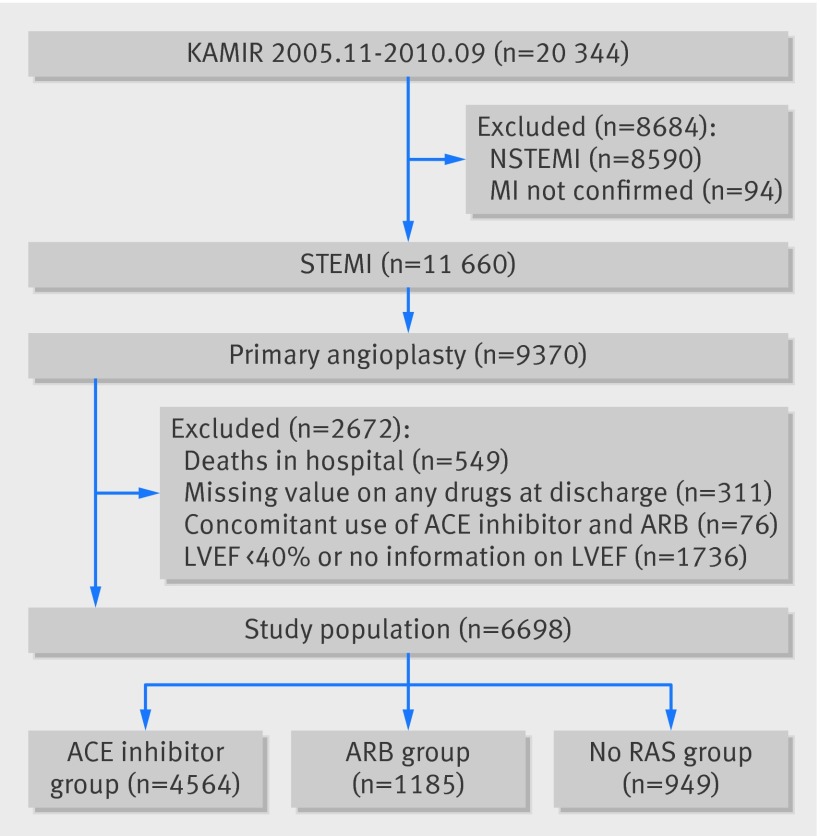
Between November 2005 and September 2010, we studied 6698 patients with ST segment elevation myocardial infarction who underwent primary percutaneous coronary intervention and had a left ventricular ejection fraction ≥ 40%.
Cardiac death or myocardial infarction. Patients were divided into an angiotensin receptor blocker group (n=1185), an angiotensin converting enzyme (ACE) inhibitor group (n=4564), and a group who did not receive any renin angiotensin system blocker (n=949). Propensity score matching analysis was also performed.
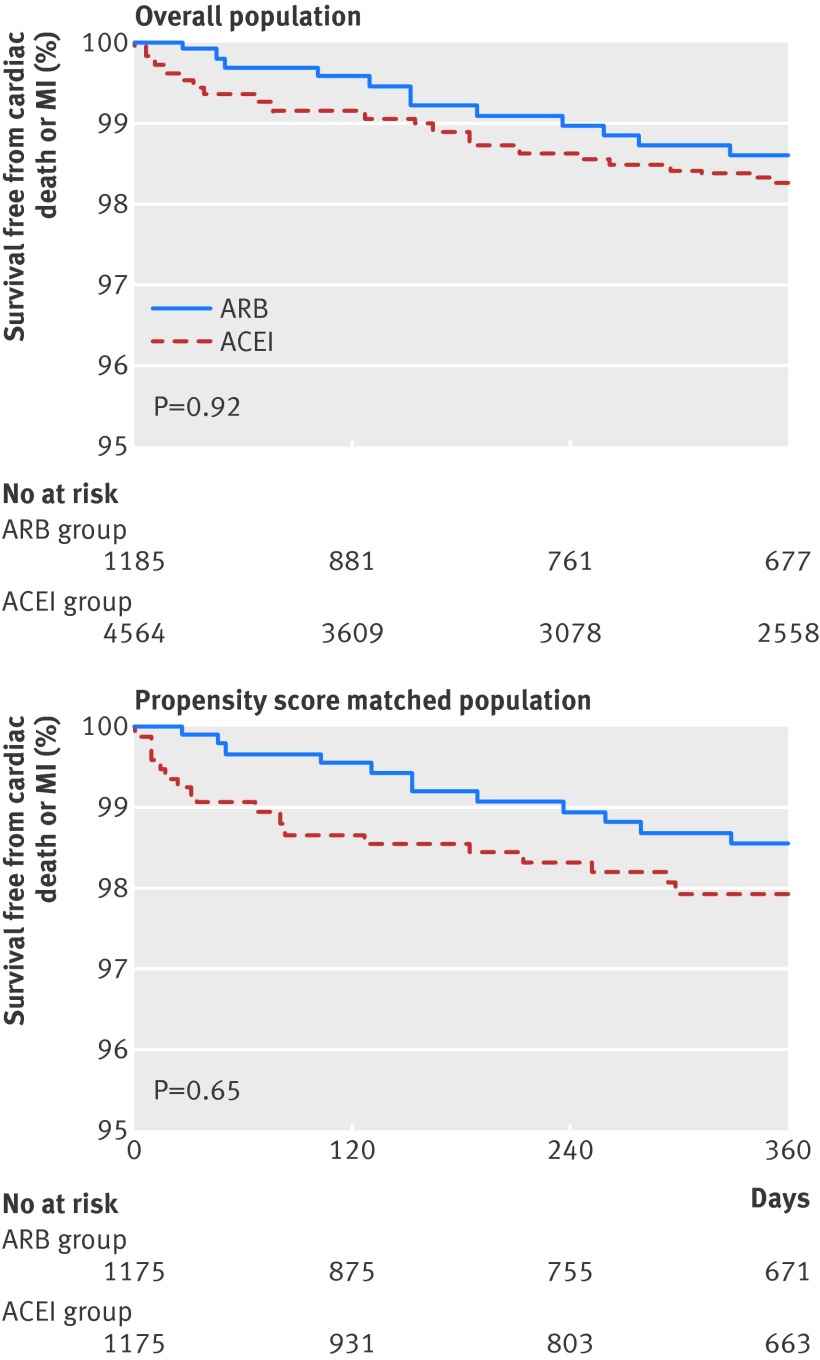
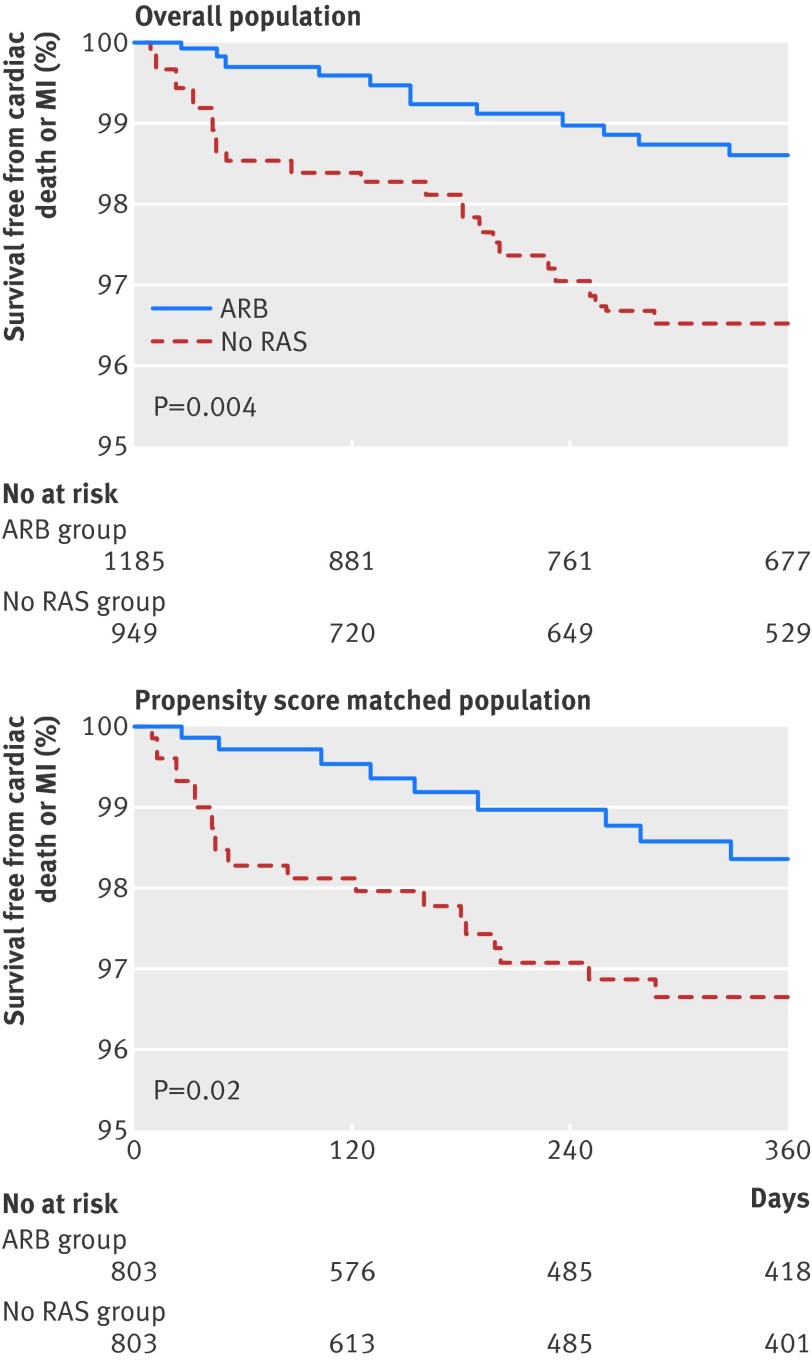
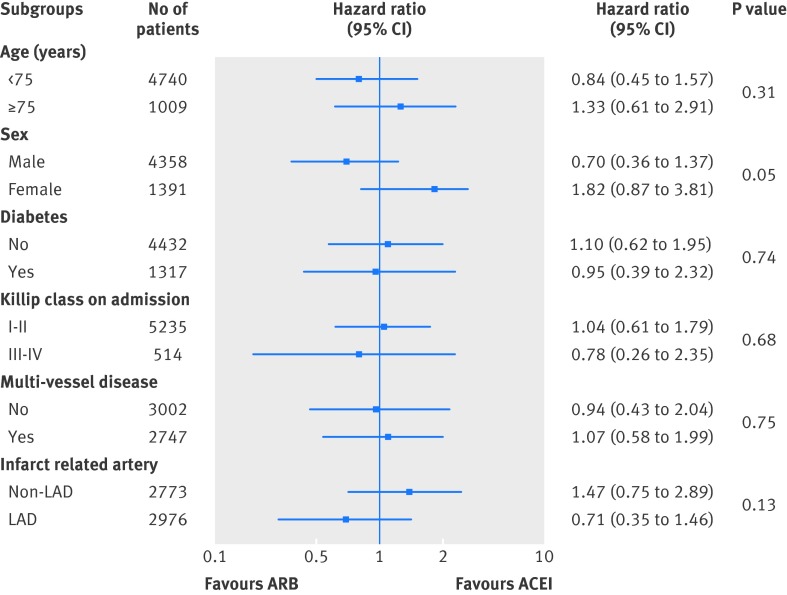
Cardiac death or myocardial infarction occurred in 21 patients (1.8%) in the angiotensin receptor blocker group, 77 patients (1.7%) in the ACE inhibitor group, and 33 patients (3.5%) in the no renin angiotensin system blocker group. After propensity score matching (1175 pairs), there was no significant difference in the rate of cardiac death or myocardial infarction between the angiotensin receptor blocker group and ACE inhibitor group (21 (1.8%) v 23 (2.0%), adjusted hazard ratio 0.65, 95% confidence interval 0.30 to 1.38; P=0.65). The angiotensin receptor blocker group had a lower rate of cardiac death or myocardial infarction than the no renin angiotensin system blocker group in matched populations (803 pairs) (14 (1.7%) v 25 (3.1%), 0.35, 0.14 to 0.90; P=0.03).
Angiotensin receptor blocker showed beneficial effects comparable with ACE inhibitors in patients with ST segment elevation myocardial infarction with preserved left ventricular systolic function. Angiotensin receptor blockers could be used as an alternative to ACE inhibitors in such patients.
探讨血管紧张素受体阻滞剂治疗与左心室收缩功能保留的ST段抬高型心肌梗死患者临床结局之间的关联。
一项使用全国大规模登记数据的前瞻性队列研究。
韩国53家参与急性心肌梗死治疗的医院。
2005年11月至2010年9月期间,我们研究了6698例接受直接经皮冠状动脉介入治疗且左心室射血分数≥40%的ST段抬高型心肌梗死患者。
心源性死亡或心肌梗死。患者分为血管紧张素受体阻滞剂组(n = 1185)、血管紧张素转换酶(ACE)抑制剂组(n = 4564)和未接受任何肾素血管紧张素系统阻滞剂的组(n = 949)。还进行了倾向评分匹配分析。
血管紧张素受体阻滞剂组有21例患者(1.8%)发生心源性死亡或心肌梗死,ACE抑制剂组有77例患者(1.7%),未接受肾素血管紧张素系统阻滞剂组有33例患者(3.5%)。倾向评分匹配(1175对)后,血管紧张素受体阻滞剂组和ACE抑制剂组的心源性死亡或心肌梗死发生率无显著差异(21例(1.8%)对23例(2.0%),调整后风险比0.65,95%置信区间0.30至1.38;P = 0.65)。在匹配人群(803对)中,血管紧张素受体阻滞剂组的心源性死亡或心肌梗死发生率低于未接受肾素血管紧张素系统阻滞剂组(14例(1.7%)对25例(3.1%),0.35,0.14至0.90;P = 0.03)。
血管紧张素受体阻滞剂在左心室收缩功能保留的ST段抬高型心肌梗死患者中显示出与ACE抑制剂相当的有益效果。在此类患者中,血管紧张素受体阻滞剂可作为ACE抑制剂的替代药物使用。