Mauri Laura, Kereiakes Dean J, Yeh Robert W, Driscoll-Shempp Priscilla, Cutlip Donald E, Steg P Gabriel, Normand Sharon-Lise T, Braunwald Eugene, Wiviott Stephen D, Cohen David J, Holmes David R, Krucoff Mitchell W, Hermiller James, Dauerman Harold L, Simon Daniel I, Kandzari David E, Garratt Kirk N, Lee David P, Pow Thomas K, Ver Lee Peter, Rinaldi Michael J, Massaro Joseph M
The authors' affiliations are listed in the Appendix.
N Engl J Med. 2014 Dec 4;371(23):2155-66. doi: 10.1056/NEJMoa1409312. Epub 2014 Nov 16.
Dual antiplatelet therapy is recommended after coronary stenting to prevent thrombotic complications, yet the benefits and risks of treatment beyond 1 year are uncertain.
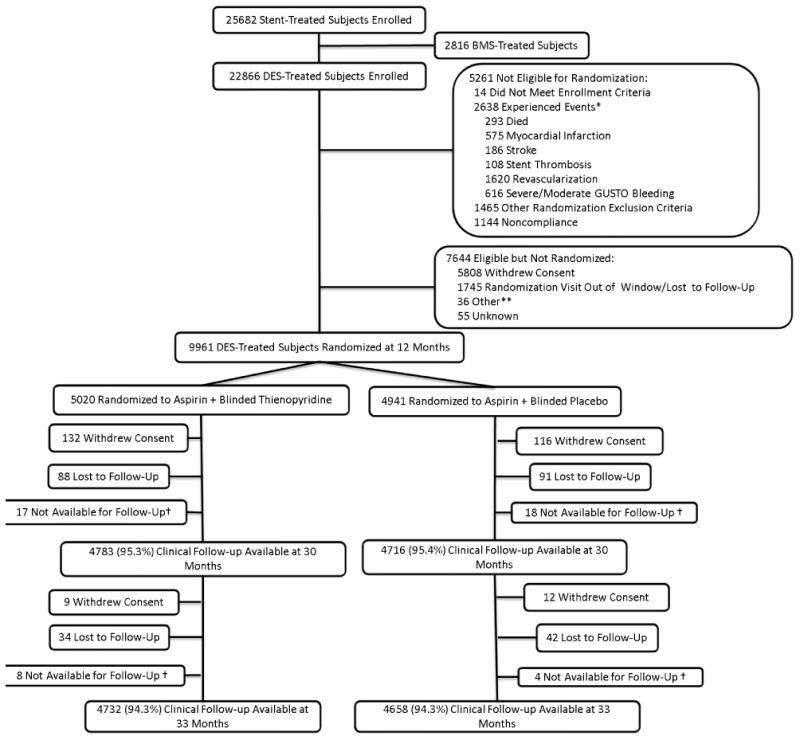
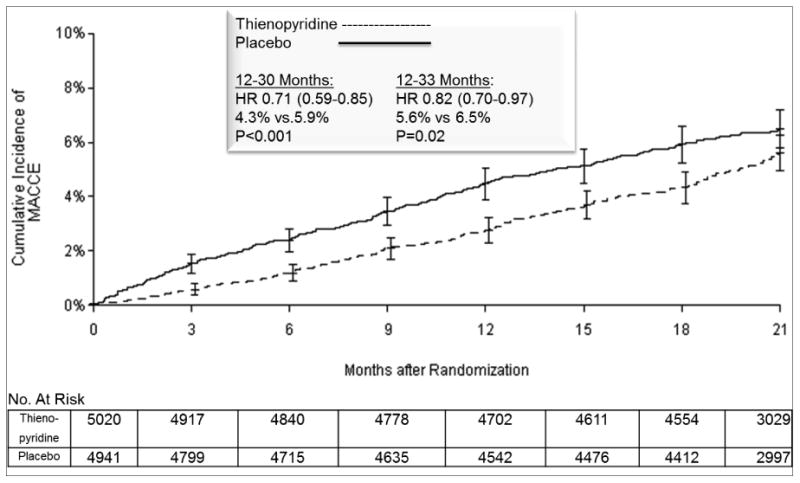
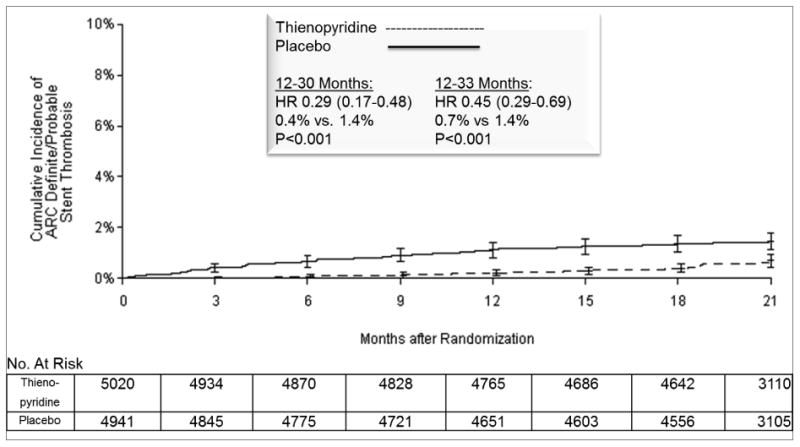
Patients were enrolled after they had undergone a coronary stent procedure in which a drug-eluting stent was placed. After 12 months of treatment with a thienopyridine drug (clopidogrel or prasugrel) and aspirin, patients were randomly assigned to continue receiving thienopyridine treatment or to receive placebo for another 18 months; all patients continued receiving aspirin. The coprimary efficacy end points were stent thrombosis and major adverse cardiovascular and cerebrovascular events (a composite of death, myocardial infarction, or stroke) during the period from 12 to 30 months. The primary safety end point was moderate or severe bleeding.
A total of 9961 patients were randomly assigned to continue thienopyridine treatment or to receive placebo. Continued treatment with thienopyridine, as compared with placebo, reduced the rates of stent thrombosis (0.4% vs. 1.4%; hazard ratio, 0.29 [95% confidence interval {CI}, 0.17 to 0.48]; P<0.001) and major adverse cardiovascular and cerebrovascular events (4.3% vs. 5.9%; hazard ratio, 0.71 [95% CI, 0.59 to 0.85]; P<0.001). The rate of myocardial infarction was lower with thienopyridine treatment than with placebo (2.1% vs. 4.1%; hazard ratio, 0.47; P<0.001). The rate of death from any cause was 2.0% in the group that continued thienopyridine therapy and 1.5% in the placebo group (hazard ratio, 1.36 [95% CI, 1.00 to 1.85]; P=0.05). The rate of moderate or severe bleeding was increased with continued thienopyridine treatment (2.5% vs. 1.6%, P=0.001). An elevated risk of stent thrombosis and myocardial infarction was observed in both groups during the 3 months after discontinuation of thienopyridine treatment.
Dual antiplatelet therapy beyond 1 year after placement of a drug-eluting stent, as compared with aspirin therapy alone, significantly reduced the risks of stent thrombosis and major adverse cardiovascular and cerebrovascular events but was associated with an increased risk of bleeding. (Funded by a consortium of eight device and drug manufacturers and others; DAPT ClinicalTrials.gov number, NCT00977938.).
冠状动脉支架置入术后推荐双联抗血小板治疗以预防血栓形成并发症,但治疗超过1年的获益和风险尚不确定。
纳入接受冠状动脉支架置入术并植入药物洗脱支架的患者。在使用噻吩并吡啶类药物(氯吡格雷或普拉格雷)和阿司匹林治疗12个月后,患者被随机分配继续接受噻吩并吡啶类药物治疗或接受安慰剂治疗18个月;所有患者继续服用阿司匹林。共同主要疗效终点为12至30个月期间的支架血栓形成和主要不良心血管和脑血管事件(死亡、心肌梗死或卒中的复合终点)。主要安全性终点为中度或重度出血。
共有9961例患者被随机分配继续噻吩并吡啶类药物治疗或接受安慰剂治疗。与安慰剂相比,继续使用噻吩并吡啶类药物治疗降低了支架血栓形成率(0.4%对1.4%;风险比,0.29[95%置信区间{CI},0.17至0.48];P<0.001)和主要不良心血管和脑血管事件发生率(4.3%对5.9%;风险比,0.71[95%CI,0.59至0.85];P<0.001)。噻吩并吡啶类药物治疗组的心肌梗死发生率低于安慰剂组(2.1%对4.1%;风险比,0.47;P<0.001)。继续噻吩并吡啶类药物治疗组的任何原因导致的死亡率为2.0%,安慰剂组为1.5%(风险比,1.36[95%CI,1.00至1.85];P=0.05)。继续噻吩并吡啶类药物治疗会增加中度或重度出血的发生率(2.5%对1.6%,P=0.001)。在停用噻吩并吡啶类药物治疗后的3个月内,两组均观察到支架血栓形成和心肌梗死风险升高。
与单独使用阿司匹林治疗相比,药物洗脱支架置入术后超过1年的双联抗血小板治疗显著降低了支架血栓形成和主要不良心血管和脑血管事件的风险,但与出血风险增加相关。(由八家器械和药物制造商等组成的财团资助;DAPT临床试验注册号,NCT00977938。)