Kim Won Young, Kwak Myoung Kwan, Ko Byuk Sung, Yoon Jae Chol, Sohn Chang Hwan, Lim Kyoung Soo, Andersen Lars W, Donnino Michael W
Department of Emergency Medicine, Ulsan University College of Medicine, Asan Medical Center, Seoul, Korea; Department of Emergency Medicine, Seoul Medical Center, Seoul, Korea.
Department of Emergency Medicine, Seoul Medical Center, Seoul, Korea.
PLoS One. 2014 Nov 17;9(11):e112779. doi: 10.1371/journal.pone.0112779. eCollection 2014.
Emergency tracheal intubation has achieved high success and low complication rates in the emergency department (ED). The objective of this study was to evaluate the incidence of post-intubation CA and determine the clinical factors associated with this complication.
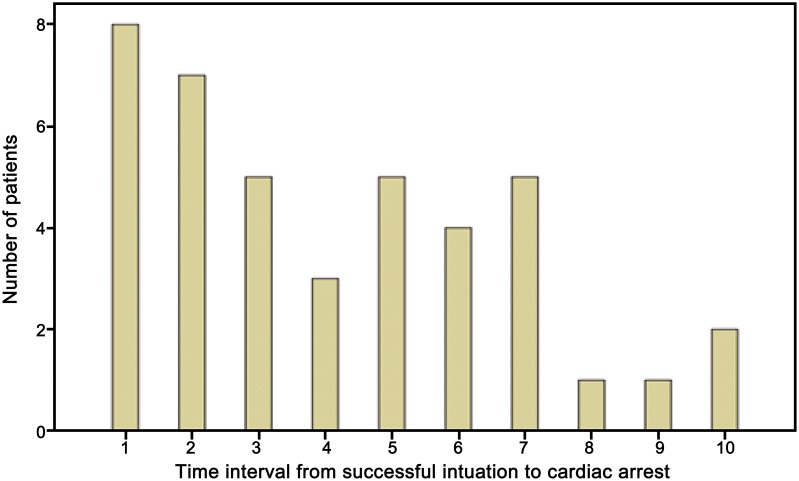
A matched case-control study with a case to control ratio of 1:3 was conducted at an urban tertiary care center between January 2007 and December 2011. Critically ill adult patients requiring emergency airway management in the ED were included. The primary endpoint was post-intubation CA, defined as CA within 10 minutes after tracheal intubation. Clinical variables were compared between patients with post-intubation CA and patients without CA who were individually matched based on age, sex, and pre-existing comorbidities.
Of 2,403 patients who underwent emergency tracheal intubation, 41 patients (1.7%) had a post-intubation CA within 10 minutes of the procedure. The most common initial rhythm was pulseless electrical activity (78.1%). Patients experiencing CA had higher in-hospital mortality than patients without CA (61.0% vs. 30.1%; p<0.001). Systolic hypotension prior to intubation, defined as a systolic blood pressure ≤ 90 mmHg, was independently associated with post-intubation CA (OR, 3.67 [95% CI, 1.58-8.55], p = 0.01).
Early post-intubation CA occurred with an approximate 2% frequency in the ED. Systolic hypotension before intubation is associated with this complication, which has potentially significant implications for clinicians at the time of intubation.
急诊气管插管在急诊科已取得较高的成功率和较低的并发症发生率。本研究的目的是评估插管后心搏骤停(CA)的发生率,并确定与该并发症相关的临床因素。
2007年1月至2011年12月期间,在一家城市三级医疗中心进行了一项病例对照研究,病例与对照的比例为1:3。纳入在急诊科需要紧急气道管理的重症成年患者。主要终点是插管后CA,定义为气管插管后10分钟内发生的CA。对插管后发生CA的患者和未发生CA的患者(根据年龄、性别和既往合并症进行个体匹配)的临床变量进行比较。
在2403例行急诊气管插管的患者中,41例(1.7%)在操作后10分钟内发生了插管后CA。最常见的初始心律是无脉电活动(78.1%)。发生CA的患者院内死亡率高于未发生CA的患者(61.0%对30.1%;p<0.001)。插管前收缩期低血压(定义为收缩压≤90 mmHg)与插管后CA独立相关(比值比,3.67[95%可信区间,1.58 - 8.55],p = 0.01)。
急诊科插管后早期CA的发生率约为2%。插管前收缩期低血压与该并发症相关,这对插管时的临床医生具有潜在的重要意义。