Visser Mieke, Deliens Luc, Houttekier Dirk
End-of-Life Care Research Group, Vrije Universiteit Brussel (VUB) and Ghent University, Laarbeeklaan 103, B-1090, Brussels, Belgium.
Department of Medical Oncology, Ghent University, De Pintelaan 185, B-9000, Ghent, Belgium.
Crit Care. 2014 Nov 18;18(6):604. doi: 10.1186/s13054-014-0604-z.
Although many terminally ill people are admitted to an intensive care unit (ICU) at the end of life, their care is often inadequate because of poor communication by physicians and lack of patient- and family-centred care. The aim of this systematic literature review was to describe physician-related barriers to adequate communication within the team and with patients and families, as well as barriers to patient- and family-centred decision-making, towards the end of life in the ICU. We base our discussion and evaluation on the quality indicators for end-of-life care in the ICU developed by the Robert Wood Johnson Foundation Critical Care End-of-Life Peer Workgroup.
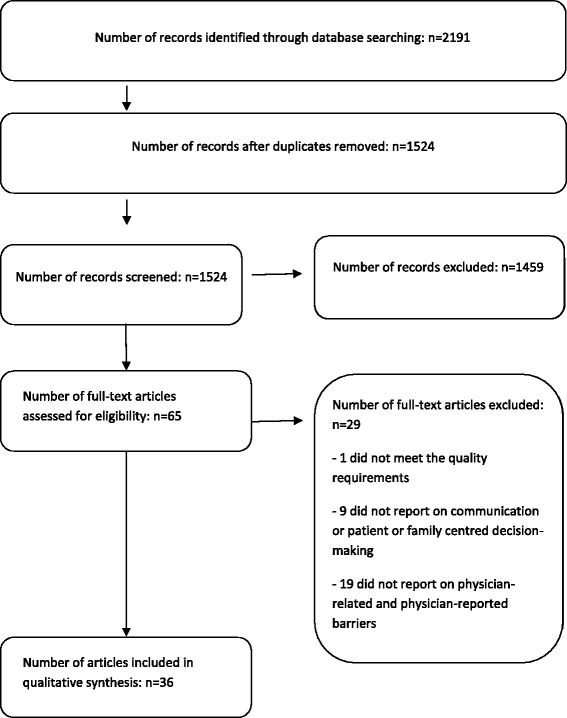
Four electronic databases (MEDLINE, Embase, CINAHL and PsycINFO) were searched, using controlled vocabulary and free text words, for potentially relevant records published between 2003 and 2013 in English or Dutch. Studies were included if the authors reported on physician-related and physician-reported barriers to adequate communication and decision-making. Barriers were categorized as being related to physicians' knowledge, physicians' attitudes or physicians' practice. Study quality was assessed using design-specific tools. Evidence for barriers was graded according to the quantity and quality of studies in which the barriers were reported.
Of 2,191 potentially relevant records, 36 studies were withheld for data synthesis. We determined 90 barriers, of which 46 were related to physicians' attitudes, 24 to physicians' knowledge and 20 to physicians' practice. Stronger evidence was found for physicians' lack of communication training and skills, their attitudes towards death in the ICU, their focus on clinical parameters and their lack of confidence in their own judgment of their patient's true condition.
We conclude that many physician-related barriers hinder adequate communication and shared decision-making in ICUs. Better physician education and palliative care guidelines are needed to enhance knowledge, attitudes and practice regarding end-of-life care. Patient-, family- and health care system-related barriers need to be examined.
尽管许多晚期患者在生命末期会被收治入重症监护病房(ICU),但由于医生沟通不善以及缺乏以患者和家庭为中心的护理,他们所接受的护理往往并不充分。本系统文献综述的目的是描述在ICU中,临近生命末期时,医生在团队内部以及与患者和家属进行充分沟通方面存在的障碍,以及以患者和家庭为中心的决策障碍。我们基于罗伯特·伍德·约翰逊基金会重症监护临终关怀同行工作组制定的ICU临终关怀质量指标进行讨论和评估。
使用受控词汇和自由文本词,检索了四个电子数据库(MEDLINE、Embase、CINAHL和PsycINFO),以查找2003年至2013年间以英文或荷兰文发表的潜在相关记录。如果作者报告了与医生相关的以及医生所报告的充分沟通和决策障碍,则纳入该研究。障碍被分类为与医生的知识、态度或实践相关。使用特定设计的工具评估研究质量。根据报告障碍的研究数量和质量对障碍证据进行分级。
在2191条潜在相关记录中,36项研究被保留用于数据合成。我们确定了90个障碍,其中46个与医生的态度有关,24个与医生的知识有关,20个与医生的实践有关。有更强的证据表明医生缺乏沟通培训和技能、他们对ICU中死亡的态度、他们对临床参数的关注以及他们对自己判断患者真实状况缺乏信心。
我们得出结论,许多与医生相关的障碍阻碍了ICU中的充分沟通和共同决策。需要更好的医生教育和姑息治疗指南,以提高关于临终关怀的知识、态度和实践。与患者、家庭和医疗保健系统相关的障碍也需要进行研究。