Ruilope Luis, Hanefeld Markolf, Lincoff A Michael, Viberti Giancarlo, Meyer-Reigner Sylvie, Mudie Nadejda, Wieczorek Kirk Dominika, Malmberg Klas, Herz Matthias
Hospital 12 de Octubre, Clinical Science, Madrid, Spain.
BMC Nephrol. 2014 Nov 18;15:180. doi: 10.1186/1471-2369-15-180.
Type 2 diabetes is a major risk factor for chronic kidney disease, which substantially increases the risk of cardiovascular disease mortality. This Phase IIb safety study (AleNephro) in patients with stage 3 chronic kidney disease and type 2 diabetes, evaluated the renal effects of aleglitazar, a balanced peroxisome proliferator-activated receptor-α/γ agonist.
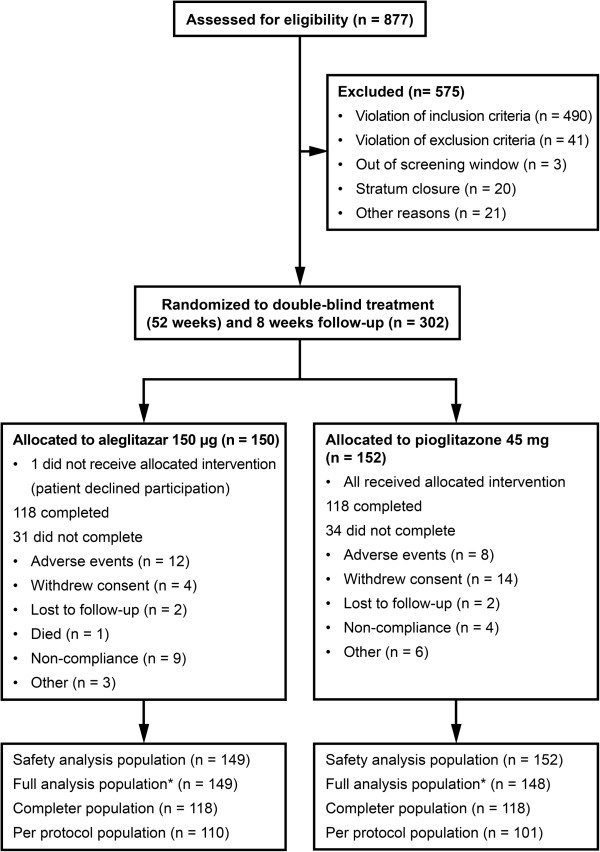
Patients were randomized to 52 weeks' double-blind treatment with aleglitazar 150 μg/day (n=150) or pioglitazone 45 mg/day (n=152), followed by an 8-week off-treatment period. The primary endpoint was non-inferiority for the difference between aleglitazar and pioglitazone in percentage change in estimated glomerular filtration rate from baseline to end of follow-up. Secondary endpoints included change from baseline in estimated glomerular filtration rate and lipid profiles at end of treatment.
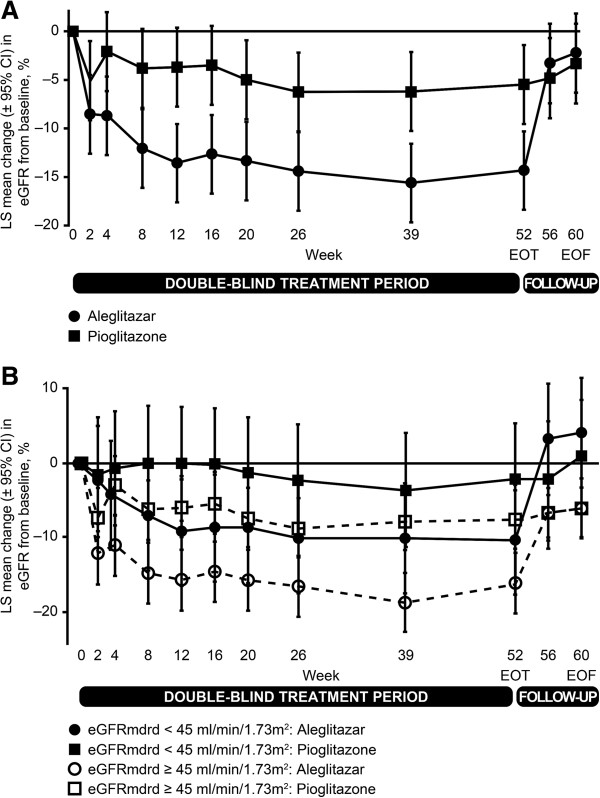
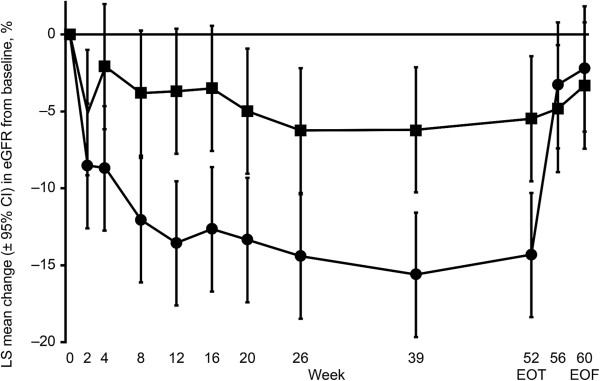
Mean estimated glomerular filtration rate change from baseline to end of follow-up was -2.7% (95% confidence interval: -7.7, 2.4) with aleglitazar versus -3.4% (95% confidence interval: -8.5, 1.7) with pioglitazone, establishing non-inferiority (0.77%; 95% confidence interval: -4.5, 6.0). Aleglitazar was associated with a 15% decrease in estimated glomerular filtration rate versus 5.4% with pioglitazone at end of treatment, which plateaued to 8 weeks and was not progressive. Superior improvements in high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and triglycerides, with similar effects on glycosylated hemoglobin were observed with aleglitazar versus pioglitazone. No major safety concerns were identified.
The primary endpoint in AleNephro was met, indicating that in stage 3 chronic kidney disease patients with type 2 diabetes, the decrease in estimated glomerular filtration rate after 52 weeks' treatment with aleglitazar followed by 8 weeks off-treatment was reversible and comparable (non-inferior) to pioglitazone.
NCT01043029 January 5, 2010.
2型糖尿病是慢性肾脏病的主要危险因素,会大幅增加心血管疾病死亡风险。这项针对3期慢性肾脏病合并2型糖尿病患者的IIb期安全性研究(AleNephro),评估了平衡型过氧化物酶体增殖物激活受体-α/γ激动剂阿格列扎的肾脏效应。
患者被随机分配接受为期52周的双盲治疗,其中150μg/天阿格列扎组(n = 150)或45mg/天吡格列酮组(n = 152),随后是为期8周的停药期。主要终点是阿格列扎与吡格列酮在估计肾小球滤过率从基线到随访结束的百分比变化差异方面的非劣效性。次要终点包括治疗结束时估计肾小球滤过率相对于基线的变化以及血脂谱。
阿格列扎组从基线到随访结束时估计肾小球滤过率的平均变化为-2.7%(95%置信区间:-7.7,2.4),吡格列酮组为-3.4%(95%置信区间:-8.5,1.7),确立了非劣效性(0.77%;95%置信区间:-4.5,6.0)。治疗结束时,阿格列扎组估计肾小球滤过率下降15%,吡格列酮组下降5.4%,下降趋势在8周时趋于平稳且无进展。与吡格列酮相比,阿格列扎在高密度脂蛋白胆固醇、低密度脂蛋白胆固醇和甘油三酯方面有更显著改善,对糖化血红蛋白的影响相似。未发现重大安全问题。
AleNephro研究达到了主要终点,表明在3期慢性肾脏病合并2型糖尿病患者中,接受52周阿格列扎治疗后停药8周,估计肾小球滤过率的下降是可逆的,且与吡格列酮相当(非劣效)。
NCT01043029,2010年1月5日。