National Health and Medical Research Council Clinical Trials Centre, University of Sydney, Sydney, New South Wales, Australia.
Diabetes Care. 2012 Feb;35(2):218-25. doi: 10.2337/dc11-1109. Epub 2011 Dec 30.
Diabetic patients with moderate renal impairment (estimated glomerular filtration rate [eGFR] 30-59 mL/min/1.73 m(2)) are at particular cardiovascular risk. Fenofibrate's safety in these patients is an issue because it may elevate plasma creatinine. Furthermore, guidelines regarding fenofibrate dosing in renal impairment vary internationally. We investigated fenofibrate's effects on cardiovascular and end-stage renal disease (ESRD) events, according to eGFR, in the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study.
Type 2 diabetic patients (aged 50-75 years) with eGFR ≥30 mL/min/1.73 m(2) were randomly allocated to a fixed dose of fenofibrate (200 mg daily) (n = 4,895) or placebo (n = 4,900) for 5 years. Baseline renal function (Modification of Diet in Renal Disease equation) was grouped by eGFR (30-59, 60-89, and ≥90 mL/min/1.73 m(2)). The prespecified outcome was total cardiovascular events (composite of cardiovascular death, myocardial infarction, stroke, and coronary/carotid revascularization). Serious adverse events and instances of ESRD (plasma creatinine >400 μmol/L, dialysis, renal transplant, or renal death) were recorded. Analysis was by intention to treat.
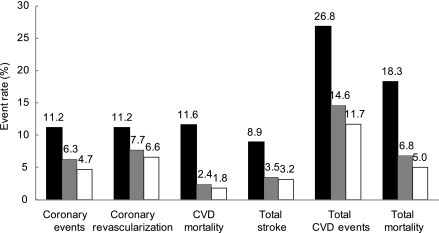
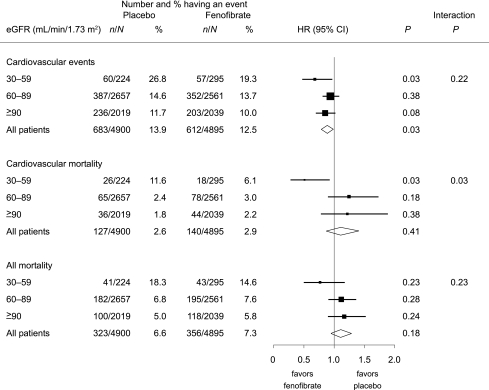
Overall, fenofibrate reduced total cardiovascular events, compared with placebo (hazard ratio 0.89 [95% CI 0.80-0.99]; P = 0.035). This benefit was not statistically different across eGFR groupings (P = 0.2 for interaction) (eGFR 30-59 mL/min/1.73 m(2): 0.68 [0.47-0.97], P = 0.035; eGFR ≥90 mL/min/1.73 m(2): 0.85 [0.70-1.02], P = 0.08). ESRD rates were similar between treatment arms, without adverse safety signals of fenofibrate use in renal impairment.
Patients with type 2 diabetes and moderate renal impairment benefit from long-term fenofibrate, without excess drug-related safety concerns compared with those with no or mild renal impairment. Fenofibrate treatment should not be contraindicated in moderate renal impairment, suggesting that current guidelines may be too restrictive.
患有中度肾功能损害(估算肾小球滤过率[eGFR]为 30-59 mL/min/1.73 m²)的糖尿病患者存在特殊的心血管风险。由于可能会升高血浆肌酐,因此,关于在这些患者中使用非诺贝特的安全性是一个问题。此外,国际上关于肾功能损害中非诺贝特剂量的指南也有所不同。我们根据 eGFR 研究了在 Fenofibrate Intervention and Event Lowering in Diabetes(FIELD)研究中,非诺贝特对心血管和终末期肾脏疾病(ESRD)事件的影响。
年龄在 50-75 岁之间、eGFR≥30 mL/min/1.73 m²的 2 型糖尿病患者被随机分配接受固定剂量的非诺贝特(每日 200 mg)(n=4895)或安慰剂(n=4900),治疗 5 年。根据 eGFR(30-59、60-89 和≥90 mL/min/1.73 m²)对肾脏功能(改良肾脏病饮食研究方程)进行分组。预先规定的结局是全因心血管事件(心血管死亡、心肌梗死、卒中和冠状动脉/颈动脉血运重建的复合结局)。记录严重不良事件和 ESRD 事件(血浆肌酐>400 μmol/L、透析、肾移植或肾死亡)。分析是按意向治疗进行的。
总体而言,与安慰剂相比,非诺贝特降低了全因心血管事件(风险比 0.89[95%CI 0.80-0.99];P=0.035)。这种益处与 eGFR 分组无统计学差异(交互作用 P=0.2)(eGFR 30-59 mL/min/1.73 m²:0.68[0.47-0.97],P=0.035;eGFR≥90 mL/min/1.73 m²:0.85[0.70-1.02],P=0.08)。治疗组之间的 ESRD 发生率相似,没有非诺贝特在肾功能损害中的不良安全信号。
与没有或轻度肾功能损害的患者相比,患有 2 型糖尿病和中度肾功能损害的患者长期使用非诺贝特获益,且药物相关安全性问题并不突出。在中度肾功能损害中不应禁忌使用非诺贝特,这表明目前的指南可能过于严格。