Roberts Ian, Coats Timothy, Edwards Phil, Gilmore Ian, Jairath Vipul, Ker Katharine, Manno Daniela, Shakur Haleema, Stanworth Simon, Veitch Andrew
Clinical Trials Unit, London School of Hygiene & Tropical Medicine, Keppel Street, London WC1E 7HT, UK.
Trials. 2014 Nov 19;15:450. doi: 10.1186/1745-6215-15-450.
Gastrointestinal bleeding is a common emergency that causes substantial mortality worldwide. Acute upper and lower gastrointestinal bleeding accounts for about 75,000 hospital admissions each year in the UK and causes the death of about 10% of these patients. Tranexamic acid has been shown to reduce the need for blood transfusion in surgical patients and to reduce mortality in bleeding trauma patients, with no apparent increase in thromboembolic events. A systematic review of clinical trials of upper gastrointestinal bleeding shows a reduction in the risk of death with tranexamic acid but the quality of the trials was poor and the estimates are imprecise. The trials were also too small to assess the effect of tranexamic acid on thromboembolic events.
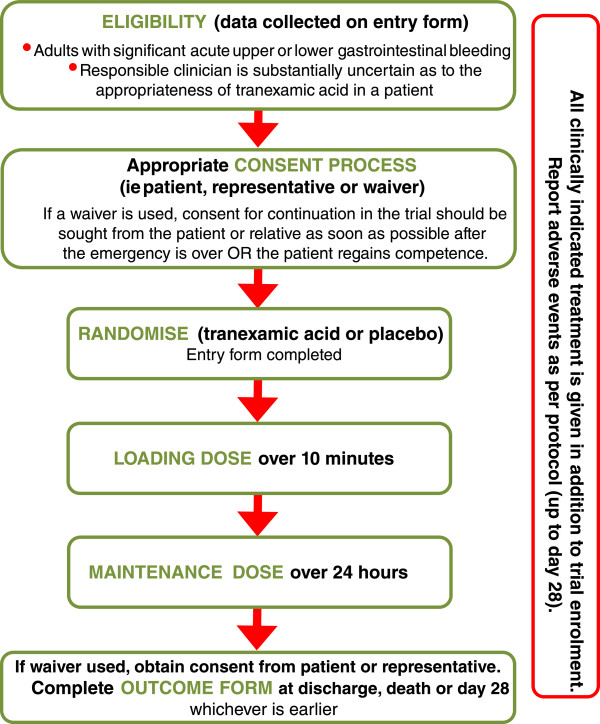
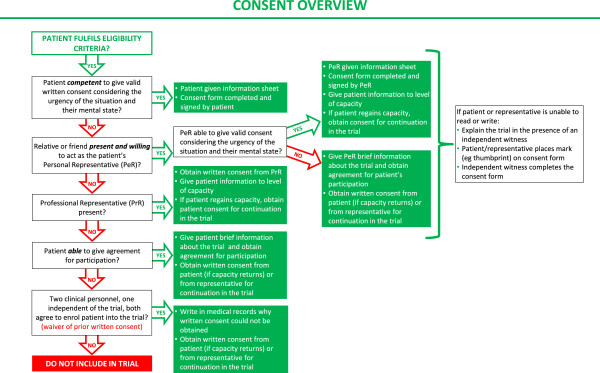
HALT-IT is a pragmatic, randomised, double-blind, placebo-controlled trial which will determine the effect of tranexamic acid on mortality, morbidity (re-bleeding, non-fatal vascular events), blood transfusion, surgical intervention, and health status in patients with acute gastrointestinal bleeding. Eight thousand adult patients who fulfil the eligibility criteria will be randomised to receive tranexamic acid or placebo. Adults with significant acute upper or lower gastrointestinal bleeding can be included if the responsible doctor is substantially uncertain as to whether or not to use tranexamic acid in that particular patient. Trial treatment consists of a loading dose of tranexamic acid (1 g by intravenous injection) or placebo (sodium chloride 0.9%) given as soon as possible after randomisation, followed by an intravenous infusion of 3 g tranexamic acid or placebo (sodium chloride 0.9%) over 24 hours. The main analyses will compare those allocated tranexamic acid with those allocated placebo, on an intention-to-treat basis. Results will be presented as effect estimates with a measure of precision (95% confidence intervals). Subgroup analyses for the primary outcome will be based on time to treatment, source of bleeding (upper versus lower), suspected variceal bleeding and severity of bleeding. A study with 8,000 patients will have over 90% power to detect a 25% reduction in mortality from 10% to 7.5%.
Current Controlled Trials ISRCTN11225767 (registration date: 3 July 2012); Clinicaltrials.gov NCT01658124 (registration date: 26 July 2012).
胃肠道出血是一种常见的急症,在全球范围内导致大量死亡。在英国,急性上消化道和下消化道出血每年导致约75000例住院病例,并导致约10%的患者死亡。氨甲环酸已被证明可减少外科手术患者的输血需求,并降低出血性创伤患者的死亡率,且血栓栓塞事件无明显增加。对上消化道出血临床试验的系统评价显示,氨甲环酸可降低死亡风险,但试验质量较差,估计结果不准确。这些试验规模也太小,无法评估氨甲环酸对血栓栓塞事件的影响。
HALT-IT是一项实用的随机双盲安慰剂对照试验,将确定氨甲环酸对急性胃肠道出血患者的死亡率、发病率(再出血、非致命性血管事件)、输血、手术干预和健康状况的影响。符合入选标准的8000名成年患者将被随机分配接受氨甲环酸或安慰剂。如果负责医生对特定患者是否使用氨甲环酸存在很大不确定性,则患有严重急性上消化道或下消化道出血的成年人可被纳入。试验治疗包括在随机分组后尽快给予氨甲环酸负荷剂量(静脉注射1g)或安慰剂(0.9%氯化钠),随后在24小时内静脉输注3g氨甲环酸或安慰剂(0.9%氯化钠)。主要分析将在意向性治疗基础上比较分配到氨甲环酸组和分配到安慰剂组的患者。结果将以带有精确性测量值(95%置信区间)的效应估计值呈现。主要结局的亚组分析将基于治疗时间、出血来源(上消化道与下消化道)、疑似静脉曲张出血和出血严重程度。一项纳入8000名患者的研究将有超过90%的把握度检测到死亡率从10%降低25%至7.5%。
当前受控试验ISRCTN11225767(注册日期:2012年7月3日);Clinicaltrials.gov NCT01658124(注册日期:2012年7月26日)。