Naeije Robert, Manes Alessandra
Dept of Cardiology, Erasme University Hospital, Brussels, Belgium. Dept of Experimental, Diagnostic and Specialty Medicine (DIMES), Bologna University Hospital, Bologna, Italy.
Eur Respir Rev. 2014 Dec;23(134):476-87. doi: 10.1183/09059180.00007414.
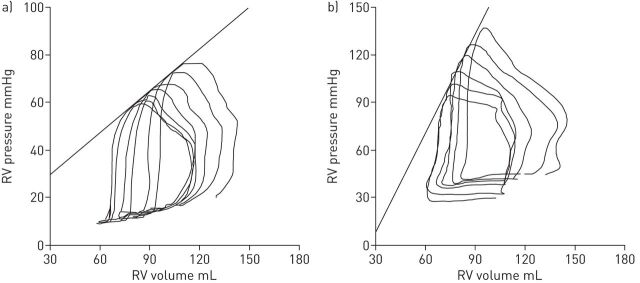
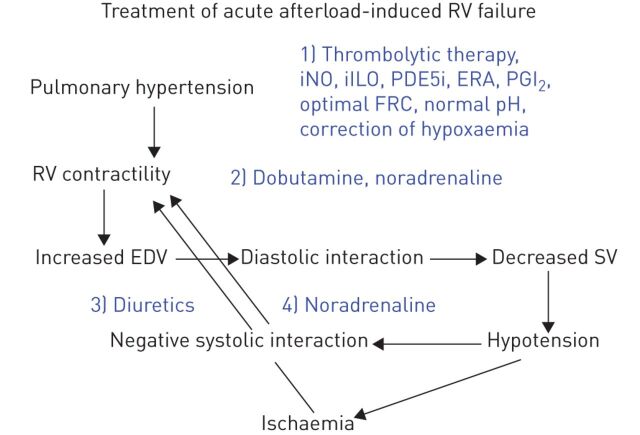
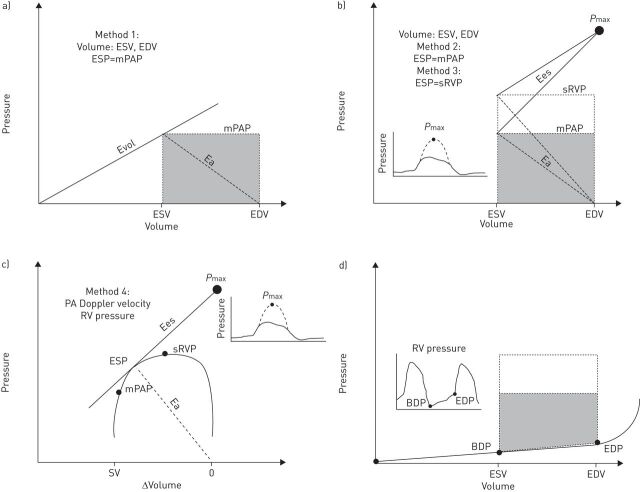
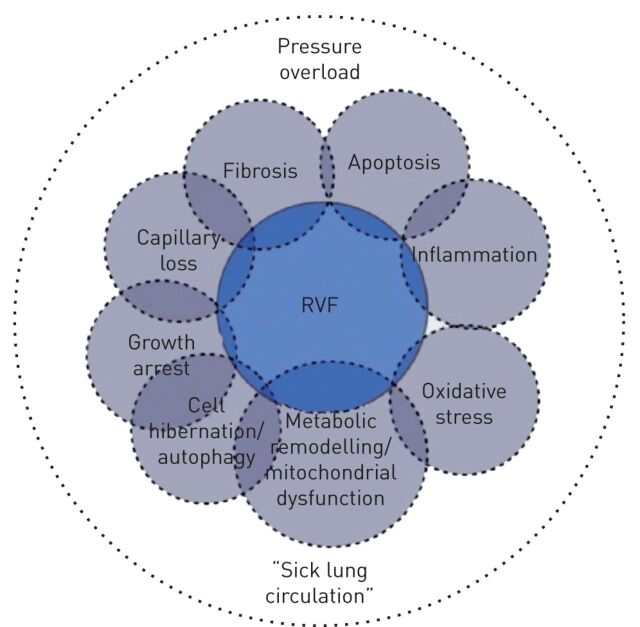
Pulmonary arterial hypertension (PAH) is a right heart failure syndrome. In early-stage PAH, the right ventricle tends to remain adapted to afterload with increased contractility and little or no increase in right heart chamber dimensions. However, less than optimal right ventricular (RV)-arterial coupling may already cause a decreased aerobic exercise capacity by limiting maximum cardiac output. In more advanced stages, RV systolic function cannot remain matched to afterload and dilatation of the right heart chamber progressively develops. In addition, diastolic dysfunction occurs due to myocardial fibrosis and sarcomeric stiffening. All these changes lead to limitation of RV flow output, increased right-sided filling pressures and under-filling of the left ventricle, with eventual decrease in systemic blood pressure and altered systolic ventricular interaction. These pathophysiological changes account for exertional dyspnoea and systemic venous congestion typical of PAH. Complete evaluation of RV failure requires echocardiographic or magnetic resonance imaging, and right heart catheterisation measurements. Treatment of RV failure in PAH relies on: decreasing afterload with drugs targeting pulmonary circulation; fluid management to optimise ventricular diastolic interactions; and inotropic interventions to reverse cardiogenic shock. To date, there has been no report of the efficacy of drug treatments that specifically target the right ventricle.
肺动脉高压(PAH)是一种右心衰竭综合征。在PAH早期,右心室倾向于通过增加收缩力来适应后负荷,而右心腔尺寸很少增加或不增加。然而,不太理想的右心室(RV)-动脉耦合可能已经通过限制最大心输出量导致有氧运动能力下降。在更晚期阶段,RV收缩功能无法再与后负荷相匹配,右心腔逐渐扩张。此外,由于心肌纤维化和肌节僵硬,会出现舒张功能障碍。所有这些变化导致RV血流输出受限、右侧充盈压升高以及左心室充盈不足,最终导致体循环血压下降和心室收缩期相互作用改变。这些病理生理变化解释了PAH典型的劳力性呼吸困难和体循环静脉淤血。对RV衰竭的全面评估需要超声心动图或磁共振成像以及右心导管测量。PAH中RV衰竭的治疗依赖于:使用针对肺循环的药物降低后负荷;进行液体管理以优化心室舒张期相互作用;以及使用正性肌力药物干预来逆转心源性休克。迄今为止,尚无专门针对右心室的药物治疗疗效的报道。