Scalone Luciana, Cesana Giancarlo, Furneri Gianluca, Ciampichini Roberta, Beck-Peccoz Paolo, Chiodini Virginio, Mangioni Silvia, Orsi Emanuela, Fornari Carla, Mantovani Lorenzo Giovanni
CESP - Research Centre on Public Health, University of Milano Bicocca, Milan, Italy; CHARTA Foundation, Milan, Italy.
CESP - Research Centre on Public Health, University of Milano Bicocca, Milan, Italy.
PLoS One. 2014 Dec 3;9(12):e113741. doi: 10.1371/journal.pone.0113741. eCollection 2014.
To assess the epidemiologic and economic burden of diabetes mellitus (DM) from a longitudinal population-based study.
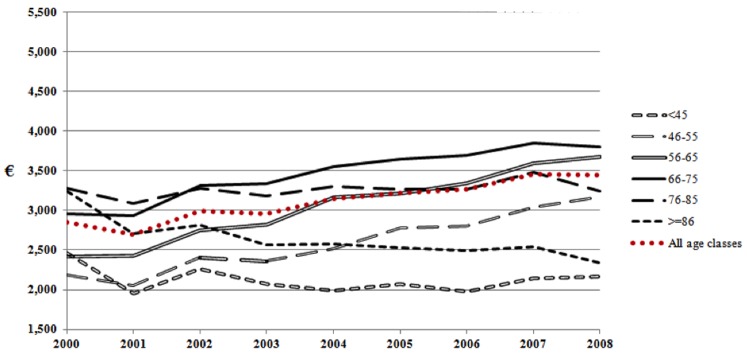
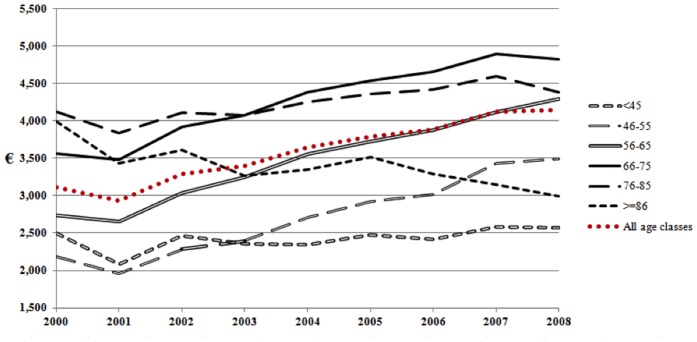
Lombardy Region includes 9.9 million individuals. Its DM population was identified through a data warehouse (DENALI), which matches with a probabilistic linkage demographic, clinical and economic data of different Healthcare Administrative databases. All individuals, who, during the year 2000 had an hospital discharge with a IDC-9 CM code 250.XX, and/or two consecutive prescriptions of drugs for diabetes (ATC code A10XXXX) within one year, and/or an exemption from co-payment healthcare costs specific for DM, were selected and followed up to 9 years. We calculated prevalence, mortality and healthcare costs (hospitalizations, drugs and outpatient examinations/visits) from the National Health Service's perspective.
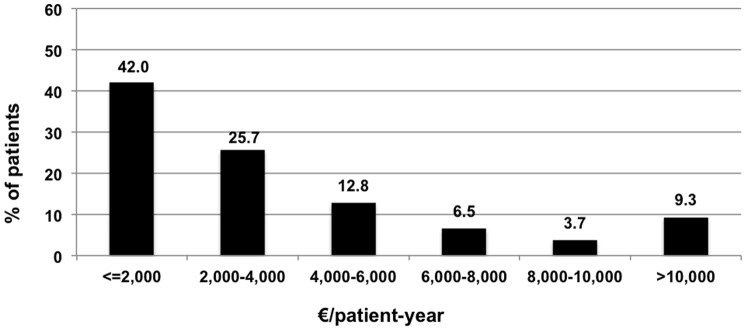
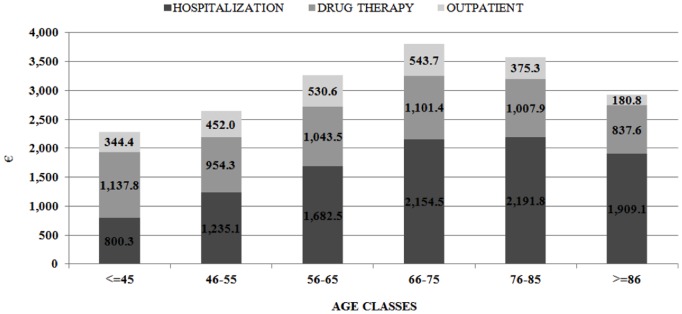
We identified 312,223 eligible subjects. The study population (51% male) had a mean age of 66 (from 0.03 to 105.12) years at the index date. Prevalence ranged from 0.4% among subjects aged ≤45 years to 10.1% among those >85 years old. Overall 43.4 deaths per 1,000 patients per year were estimated, significantly (p<0.001) higher in men than women. Overall, 3,315€/patient-year were spent on average: hospitalizations were the cost driver (54.2% of total cost). Drugs contributed to 31.5%, outpatient claims represented 14.3% of total costs. Thirty-five percent of hospital costs were attributable to cerebro-/cardiovascular reasons, 6% to other complications of DM, and 4% to DM as a main diagnosis. Cardiovascular drugs contributed to 33.5% of total drug costs, 21.8% was attributable to class A (16.7% to class A10) and 4.3% to class B (2.4% to class B01) drugs.
Merging different administrative databases can provide with many data from large populations observed for long time periods. DENALI shows to be an efficient instrument to obtain accurate estimates of burden of diseases such as diabetes mellitus.
通过一项基于人群的纵向研究评估糖尿病(DM)的流行病学和经济负担。
伦巴第大区有990万人口。其糖尿病患者群体通过一个数据仓库(DENALI)识别,该数据仓库将不同医疗保健管理数据库的人口统计学、临床和经济数据进行概率关联匹配。所有在2000年有国际疾病分类第九版临床修订本(IDC-9 CM)代码250.XX的出院记录,和/或一年内连续两次糖尿病药物处方(解剖治疗化学代码A10XXXX),和/或免除糖尿病特定的医疗费用共付额的个体被选取并随访9年。我们从国家卫生服务的角度计算患病率、死亡率和医疗费用(住院、药物和门诊检查/就诊)。
我们识别出312,223名符合条件的受试者。研究人群(51%为男性)在索引日期时的平均年龄为66岁(范围从0.03至105.12岁)。患病率在年龄≤45岁的受试者中为0.4%,在>85岁的受试者中为10.1%。估计每年每1000名患者中有43.4人死亡,男性显著高于女性(p<0.001)。总体而言,平均每位患者每年花费3315欧元:住院是成本驱动因素(占总成本的54.2%)。药物占31.5%,门诊费用占总成本的14.3%。35%的住院费用归因于脑血管/心血管原因,6%归因于糖尿病的其他并发症,4%归因于糖尿病作为主要诊断。心血管药物占药物总成本的33.5%,21.8%归因于A类(16.7%归因于A10类),4.3%归因于B类(2.4%归因于B01类)药物。
合并不同的管理数据库可以提供来自大量人群长时间观察的许多数据。DENALI被证明是获得诸如糖尿病等疾病负担准确估计的有效工具。