Salsbury Stacie A, DeVocht James W, Hondras Maria A, Seidman Michael B, Stanford Clark M, Goertz Christine M
Palmer College of Chiropractic, Palmer Center for Chiropractic Research, 741 Brady Street, Davenport, IA 52803 USA.
Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark.
Chiropr Man Therap. 2014 Dec 3;22(1):42. doi: 10.1186/s12998-014-0042-7. eCollection 2014.
Chiropractic care is a complex health intervention composed of both treatment effects and non-specific, or placebo, effects. While doctor-patient interactions are a component of the non-specific effects of chiropractic, these effects are not evaluated in most clinical trials. This study aimed to: 1) develop an instrument to assess practitioner-patient interactions; 2) determine the equivalence of a chiropractor's verbal interactions and treatment delivery for participants allocated to active or sham chiropractic groups; and 3) describe the perceptions of a treatment-masked evaluator and study participants regarding treatment group assignment.
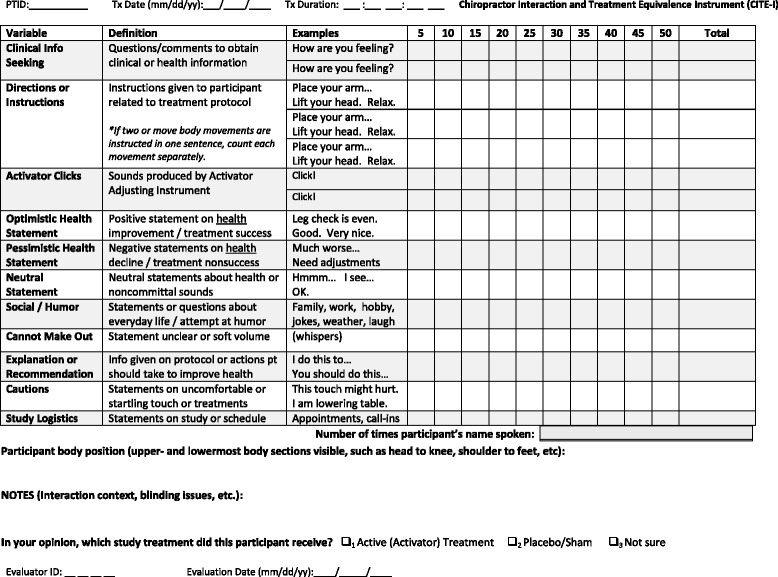
We conducted an observational analysis of digital video-recordings derived from study visits conducted during a pilot randomized trial of conservative therapies for temporomandibular pain. A theory-based, iterative process developed the 13-item Chiropractor Interaction and Treatment Equivalence Instrument. A trained evaluator masked to treatment assignment coded video-recordings of clinical encounters between one chiropractor and multiple visits of 26 participants allocated to active or sham chiropractic treatment groups. Non-parametric statistics were calculated.
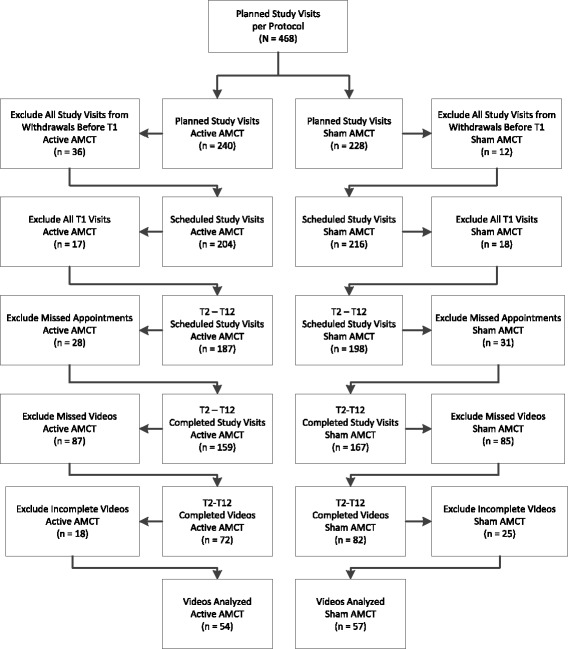
The trial ran from January 2010 to October 2011. We analyzed 111 complete video-recordings (54 active, 57 sham). Chiropractor interactions differed between the treatment groups in 7 categories. Active participants received more interactions with clinical information (8 vs. 4) or explanations (3.5 vs. 1) than sham participants within the therapeutic domain. Active participants received more directions (63 vs. 58) and adjusting instrument thrusts (41.5 vs. 23) in the procedural domain and more optimistic (2.5 vs. 0) or neutral (7.5 vs. 5) outcome statements in the treatment effectiveness domain. Active participants recorded longer visit durations (13.5 vs. 10 minutes). The evaluator correctly identified 61% of active care video-recordings as active treatments but categorized only 31% of the sham treatments correctly. Following the first treatment, 82% of active and 11% of sham participants correctly identified their treatment group. At 2-months, 93% of active and 42% of sham participants correctly identified their group assignment.
Our findings show the feasibility of evaluating doctor-patient interactions in chiropractic clinical trials using video-recordings and standardized instrumentation. Clinical trial design and clinician training protocols should improve and assess the equivalence of doctor-patient interactions between treatment groups.
This trial was registered in ClinicalTrials.gov as NCT01021306 on 24 November 2009.
整脊疗法是一种复杂的健康干预措施,由治疗效果和非特异性(即安慰剂)效应组成。虽然医患互动是非特异性整脊效应的一个组成部分,但在大多数临床试验中并未对这些效应进行评估。本研究旨在:1)开发一种工具来评估从业者与患者之间的互动;2)确定分配到整脊治疗组或假整脊治疗组的参与者所接受的脊椎按摩师言语互动和治疗操作的等效性;3)描述对治疗不知情的评估者和研究参与者对治疗组分配的看法。
我们对颞下颌疼痛保守治疗的一项试点随机试验期间研究访视的数字视频记录进行了观察性分析。一个基于理论的迭代过程开发了包含13个条目的整脊师互动与治疗等效性工具。一名对治疗分配不知情的经过培训的评估者,对一名整脊师与分配到整脊治疗组或假整脊治疗组的26名参与者的多次访视之间的临床接触视频记录进行编码。计算了非参数统计量。
该试验于2010年1月至2011年10月进行。我们分析了111份完整的视频记录(54份为整脊治疗,57份为假治疗)。整脊师的互动在7个类别上治疗组之间存在差异。在治疗领域,接受整脊治疗的参与者比接受假治疗的参与者获得了更多关于临床信息(8次对4次)或解释(3.5次对1次)的互动。在操作领域,接受整脊治疗的参与者获得了更多的指导(63次对58次)和调整器械推力(41.5次对23次),在治疗效果领域获得了更积极(2.5次对0次)或中性(7.5次对5次)的结果陈述。接受整脊治疗的参与者记录的访视时间更长(13.5分钟对10分钟)。评估者正确地将61%的整脊治疗视频记录识别为整脊治疗,但仅正确地将31%的假治疗进行了分类。在首次治疗后,82%接受整脊治疗的参与者和11%接受假治疗的参与者正确地识别了他们的治疗组。在2个月时,93%接受整脊治疗的参与者和42%接受假治疗的参与者正确地识别了他们的分组。
我们的研究结果表明,使用视频记录和标准化工具评估整脊临床试验中医患互动的可行性。临床试验设计和临床医生培训方案应改进并评估治疗组之间医患互动的等效性。
本试验于2009年11月24日在ClinicalTrials.gov上注册,注册号为NCT01021306。