Polonsky Jonathan A, Martínez-Pino Isabel, Nackers Fabienne, Chonzi Prosper, Manangazira Portia, Van Herp Michel, Maes Peter, Porten Klaudia, Luquero Francisco J
Epicentre, Paris, France.
Epicentre, Paris, France; European Programme for Intervention Epidemiology Training, European Centre for Disease Prevention and Control, Stockholm, Sweden.
PLoS One. 2014 Dec 8;9(12):e114702. doi: 10.1371/journal.pone.0114702. eCollection 2014.
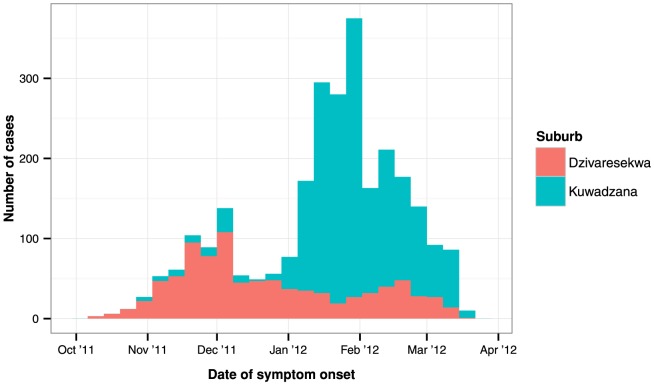
Typhoid fever remains a significant public health problem in developing countries. In October 2011, a typhoid fever epidemic was declared in Harare, Zimbabwe - the fourth enteric infection epidemic since 2008. To orient control activities, we described the epidemiology and spatiotemporal clustering of the epidemic in Dzivaresekwa and Kuwadzana, the two most affected suburbs of Harare.
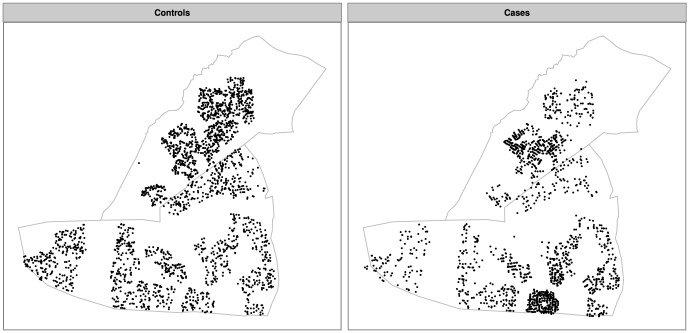
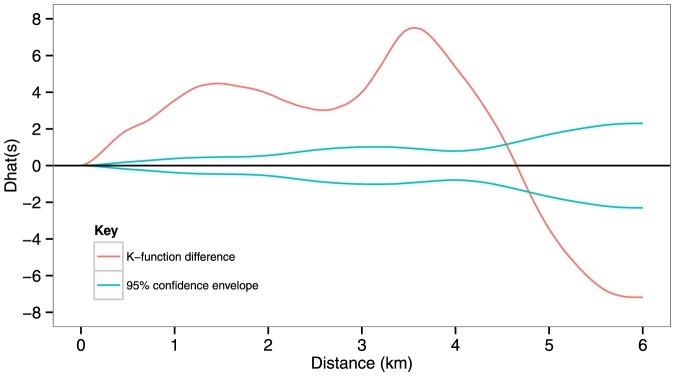
A typhoid fever case-patient register was analysed to describe the epidemic. To explore clustering, we constructed a dataset comprising GPS coordinates of case-patient residences and randomly sampled residential locations (spatial controls). The scale and significance of clustering was explored with Ripley K functions. Cluster locations were determined by a random labelling technique and confirmed using Kulldorff's spatial scan statistic.
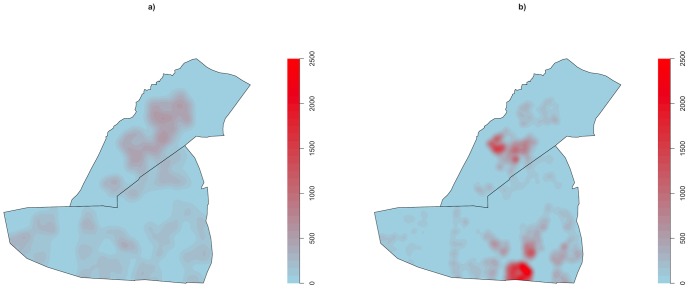
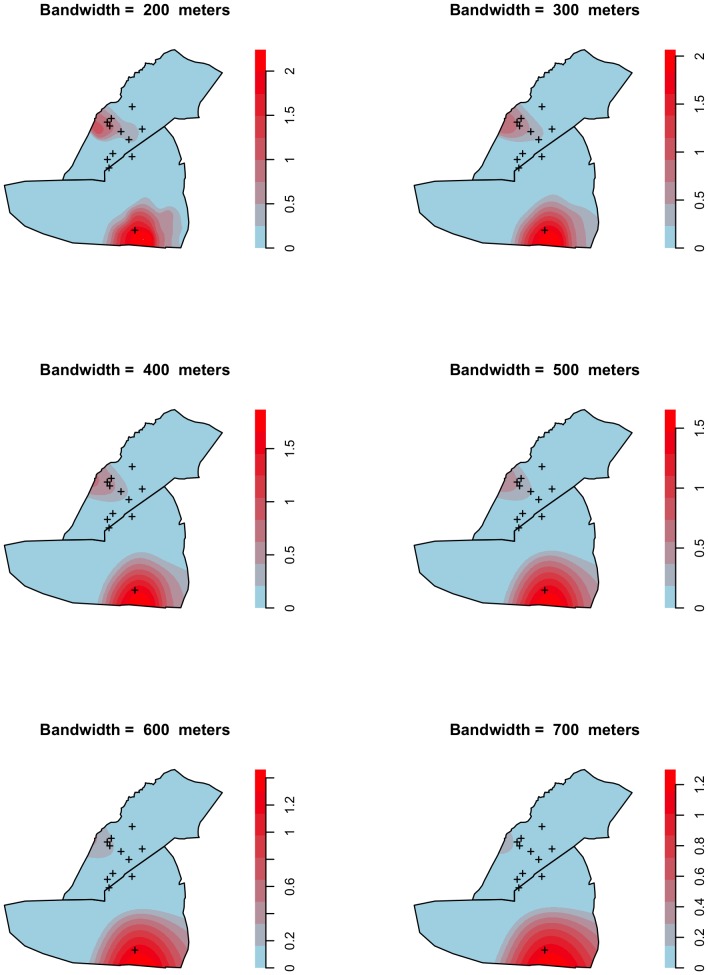
We analysed data from 2570 confirmed and suspected case-patients, and found significant spatiotemporal clustering of typhoid fever in two non-overlapping areas, which appeared to be linked to environmental sources. Peak relative risk was more than six times greater than in areas lying outside the cluster ranges. Clusters were identified in similar geographical ranges by both random labelling and Kulldorff's spatial scan statistic. The spatial scale at which typhoid fever clustered was highly localised, with significant clustering at distances up to 4.5 km and peak levels at approximately 3.5 km. The epicentre of infection transmission shifted from one cluster to the other during the course of the epidemic.
This study demonstrated highly localised clustering of typhoid fever during an epidemic in an urban African setting, and highlights the importance of spatiotemporal analysis for making timely decisions about targetting prevention and control activities and reinforcing treatment during epidemics. This approach should be integrated into existing surveillance systems to facilitate early detection of epidemics and identify their spatial range.
伤寒热在发展中国家仍然是一个重大的公共卫生问题。2011年10月,津巴布韦哈拉雷宣布爆发伤寒热疫情,这是自2008年以来的第四次肠道感染疫情。为指导防控工作,我们描述了哈拉雷受灾最严重的两个郊区Dzivaresekwa和Kuwadzana的疫情流行病学特征及时空聚集情况。
分析伤寒热病例登记册以描述疫情。为探究聚集情况,我们构建了一个数据集,其中包括病例居住地址的GPS坐标和随机抽样的居住地点(空间对照)。使用Ripley K函数探究聚集的规模和显著性。通过随机标记技术确定聚集位置,并使用Kulldorff空间扫描统计量进行确认。
我们分析了2570例确诊和疑似病例的数据,发现伤寒热在两个不重叠的区域存在显著的时空聚集,这似乎与环境源有关。相对风险峰值比聚集范围以外的地区高出六倍多。通过随机标记和Kulldorff空间扫描统计量在相似的地理范围内识别出了聚集区。伤寒热聚集的空间尺度高度局部化,在距离达4.5公里处有显著聚集,峰值水平出现在约3.5公里处。在疫情过程中,感染传播的中心从一个聚集区转移到了另一个聚集区。
本研究表明,在非洲城市环境的疫情期间,伤寒热存在高度局部化的聚集,强调了时空分析对于及时做出关于预防和控制活动目标以及在疫情期间加强治疗的决策的重要性。这种方法应纳入现有的监测系统,以促进疫情的早期发现并确定其空间范围。