Nwogu Chukwumere E, D'Cunha Jonathan, Pang Herbert, Gu Lin, Wang Xiaofei, Richards William G, Veit Linda J, Demmy Todd L, Sugarbaker David J, Kohman Leslie J, Swanson Scott J
Roswell Park Cancer Institute, State University of New York at Buffalo, Buffalo, New York.
University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
Ann Thorac Surg. 2015 Feb;99(2):399-405. doi: 10.1016/j.athoracsur.2014.09.018. Epub 2014 Dec 10.
The short-term superiority of video-assisted thoracoscopic surgery lobectomy compared with open lobectomy for early-stage lung cancer has been suggested by single-institution studies. Lack of equipoise limits the feasibility of a randomized study to confirm this. The hypothesis of this study (CALGB 31001) was that VATS lobectomy results in shorter length of hospital stay and fewer complications compared with open lobectomy in stages I and II non-small cell lung cancer in a multi-institutional setting.
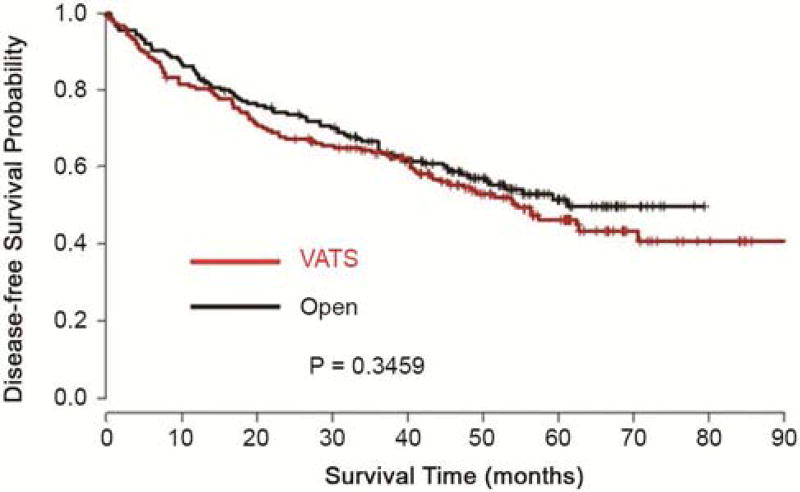
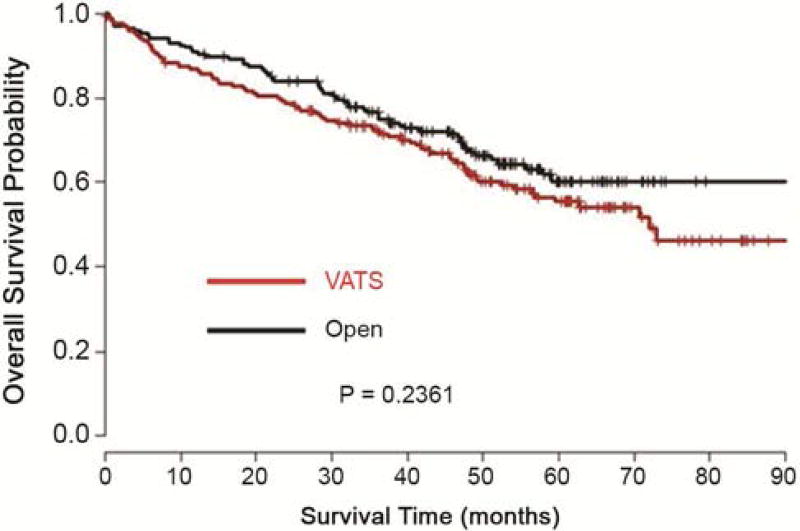
Five hundred nineteen patients whose tumors had been collected as part of CALGB 140202 (lung cancer tissue bank) were eligible. Propensity-scoring using age, race, sex, performance status, comorbidities, histology, tumor stage, and size as independent variables was used to create a 1:1 matched group of 175 pairs of patients. McNemar's test for binary variables and Wilcoxon signed-rank test for continuous variables were used to assess differences in length of hospital stay, complications, and discharge dispositions between the groups. Comparison of disease-free and overall survival between the two approaches was done using the log-rank test. Probability values of less than 0.05 were considered significant.
The matched data on length of hospital stay, complications, and discharge dispositions significantly favored the video-assisted thoracoscopic surgery group. There was no statistically significant difference in survival between the two approaches.
This multi-institutional study supports the assertion that thoracoscopic lobectomy results in shorter hospital length of stay, fewer perioperative complications, and greater likelihood of independent home discharge compared with open lobectomy for early-stage lung cancer. Survival was comparable between the two groups.
单机构研究表明,与开放性肺叶切除术相比,电视辅助胸腔镜手术肺叶切除术治疗早期肺癌具有短期优势。缺乏均衡性限制了通过随机研究来证实这一点的可行性。本研究(CALGB 31001)的假设是,在多机构环境中,对于Ⅰ期和Ⅱ期非小细胞肺癌,电视辅助胸腔镜手术肺叶切除术与开放性肺叶切除术相比,可缩短住院时间且并发症更少。
519例作为CALGB 140202(肺癌组织库)一部分收集肿瘤的患者符合条件。以年龄、种族、性别、体能状态、合并症、组织学类型、肿瘤分期和大小作为自变量进行倾向评分,以创建175对1:1匹配的患者组。使用二元变量的McNemar检验和连续变量的Wilcoxon符号秩检验来评估两组之间住院时间、并发症和出院处置的差异。采用对数秩检验比较两种手术方式的无病生存期和总生存期。概率值小于0.05被认为具有统计学意义。
在住院时间、并发症和出院处置方面的匹配数据明显有利于电视辅助胸腔镜手术组。两种手术方式在生存率方面无统计学显著差异。
这项多机构研究支持以下观点,即对于早期肺癌,与开放性肺叶切除术相比,胸腔镜肺叶切除术可缩短住院时间,减少围手术期并发症,并更有可能独立出院回家。两组的生存率相当。