Hicks Martin J, Funato Kosuke, Wang Lan, Aronowitz Eric, Dyke Jonathan P, Ballon Douglas J, Havlicek David F, Frenk Esther Z, De Bishnu P, Chiuchiolo Maria J, Sondhi Dolan, Hackett Neil R, Kaminsky Stephen M, Tabar Viviane, Crystal Ronald G
Department of Genetic Medicine Weill Cornell Medical College, New York, New York.
Department of Neurosurgery Memorial Sloan-Kettering Cancer Center, New York, New York and.
Cancer Gene Ther. 2015 Jan;22(1):1-8. doi: 10.1038/cgt.2014.58. Epub 2014 Dec 12.
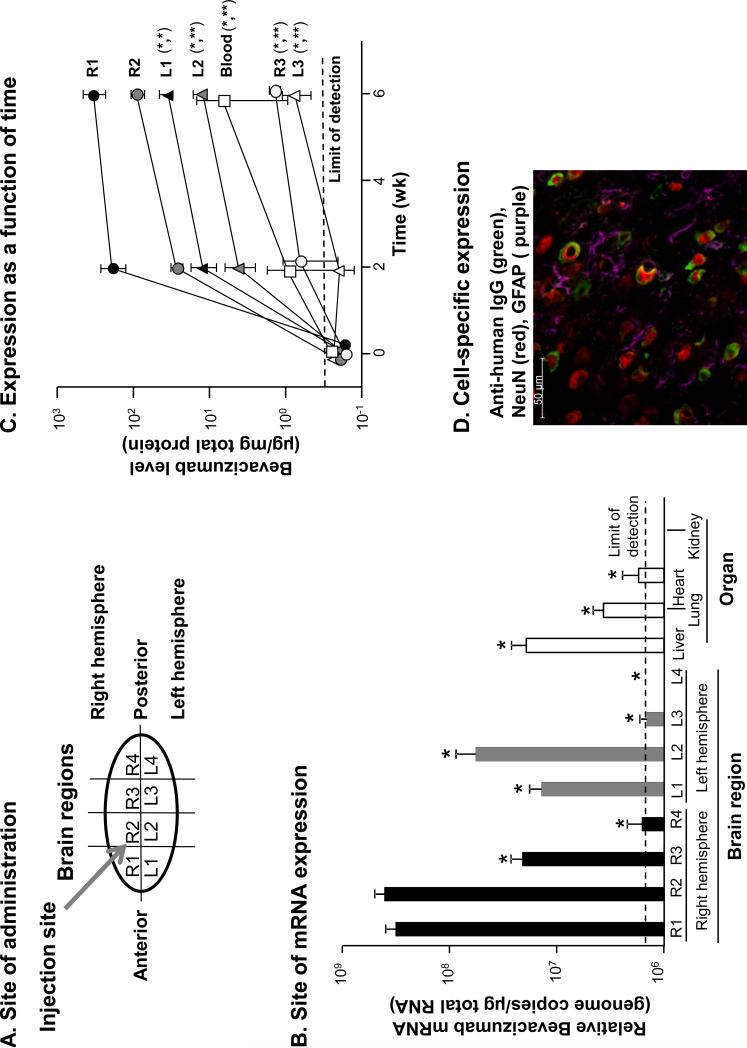
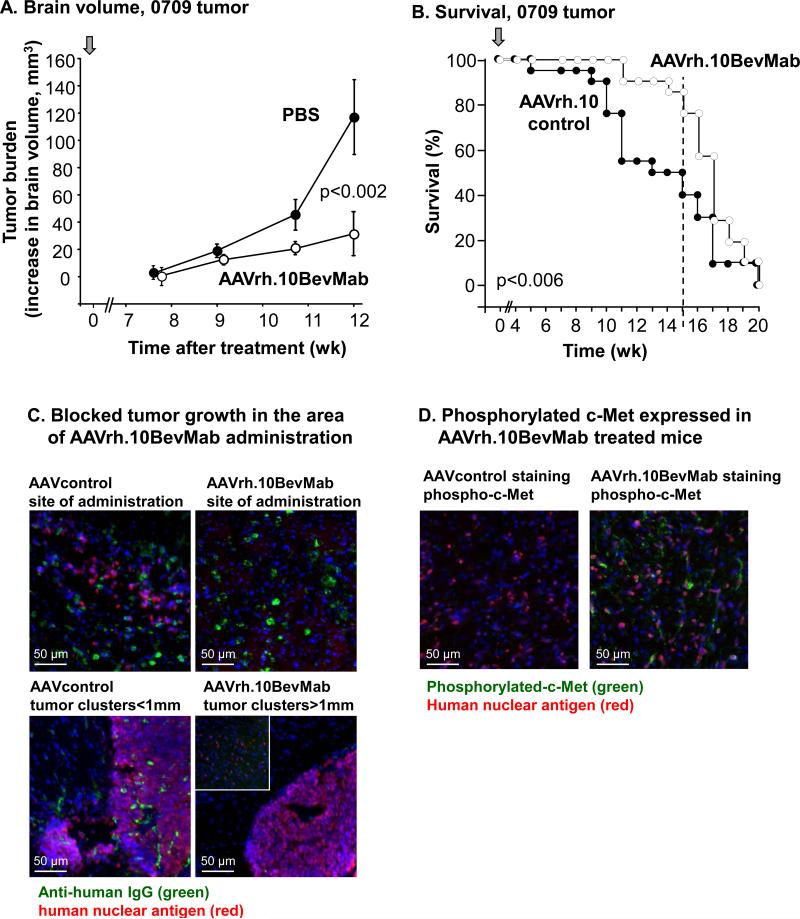
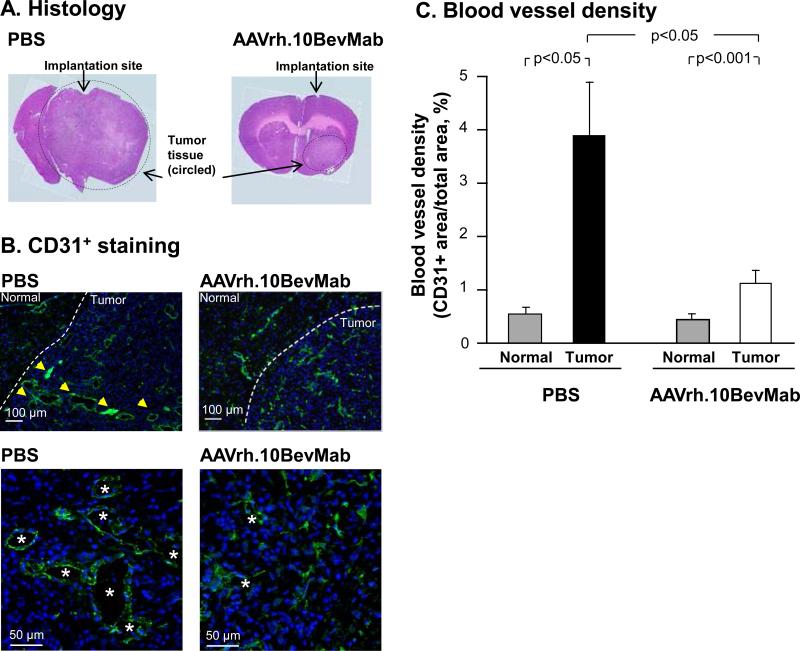
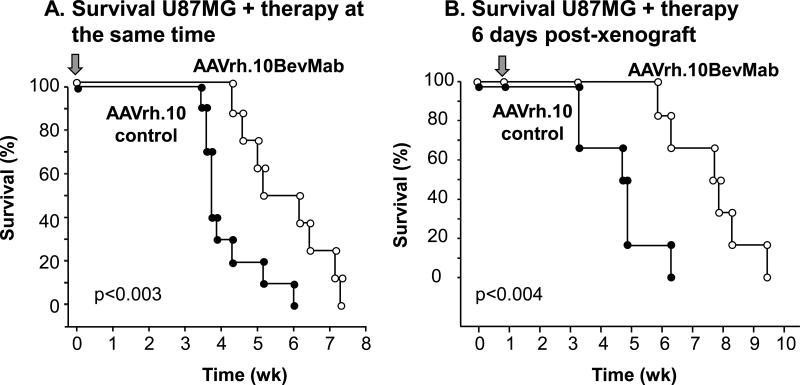
The median survival of glioblastoma multiforme (GBM) is approximately 1 year. Following surgical removal, systemic therapies are limited by the blood-brain barrier. To circumvent this, we developed a method to modify neurons with the genetic sequence for therapeutic monoclonal antibodies using adeno-associated virus (AAV) gene transfer vectors, directing persistent, local expression in the tumor milieu. The human U87MG GBM cell line or patient-derived early passage GBM cells were administered to the striatum of NOD/SCID immunodeficient mice. AAVrh.10BevMab, an AAVrh.10-based vector coding for bevacizumab (Avastin), an anti-human vascular endothelial growth factor (VEGF) monoclonal antibody, was delivered to the area of the GBM xenograft. Localized expression of bevacizumab was demonstrated by quantitative PCR, ELISA and western blotting. Immunohistochemistry showed that bevacizumab was expressed in neurons. Concurrent administration of AAVrh.10BevMab with the U87MG tumor reduced tumor blood vessel density and tumor volume, and increased survival. Administration of AAVrh.10BevMab 1 week after U87MG xenograft reduced growth and increased survival. Studies with patient-derived early passage GBM primary cells showed a reduction in primary tumor burden with an increased survival. These data support the strategy of AAV-mediated central nervous system gene therapy to treat GBM, overcoming the blood-brain barrier through local, persistent delivery of an anti-angiogenesis monoclonal antibody.
多形性胶质母细胞瘤(GBM)的中位生存期约为1年。手术切除后,全身治疗受到血脑屏障的限制。为了规避这一问题,我们开发了一种方法,利用腺相关病毒(AAV)基因转移载体,用治疗性单克隆抗体的基因序列修饰神经元,使其在肿瘤环境中持续、局部表达。将人U87MG胶质母细胞瘤细胞系或患者来源的早期传代胶质母细胞瘤细胞接种到NOD/SCID免疫缺陷小鼠的纹状体中。将编码贝伐单抗(阿瓦斯汀)的基于AAVrh.10的载体AAVrh.10BevMab(一种抗人血管内皮生长因子(VEGF)单克隆抗体)递送至胶质母细胞瘤异种移植区域。通过定量PCR、ELISA和蛋白质印迹法证实了贝伐单抗的局部表达。免疫组织化学显示贝伐单抗在神经元中表达。AAVrh.10BevMab与U87MG肿瘤同时给药可降低肿瘤血管密度和肿瘤体积,并延长生存期。在U87MG异种移植1周后给予AAVrh.10BevMab可抑制肿瘤生长并延长生存期。对患者来源的早期传代胶质母细胞瘤原代细胞的研究表明,原发性肿瘤负担减轻,生存期延长。这些数据支持了AAV介导的中枢神经系统基因治疗策略,通过局部、持续递送抗血管生成单克隆抗体来治疗GBM,克服血脑屏障。